Attenuated heart rate (HR) response during exercise is associated with adverse cardiovascular outcome. The acceptable value for HR response is 85% of the age-predicted maximal HR (APMHR). This study hypothesized that mild attenuation of HR response during exercise among healthy subjects is associated with increased cardiovascular risk. The study population comprised 10,323 healthy men and women without known cardiovascular disease (CVD) or diabetes mellitus who underwent a yearly screening program and were followed up during a mean period of 4.3 years. Participants were grouped to 3 tertiles based on the percentage of their APMHR reached at the baseline stress test. The primary end point was the occurrence of CVD or cerebrovascular disease. A total of 1,015 incident cases of CVD occurred during follow-up. A multivariate Cox proportional hazards regression model showed that the CVD risk of subjects who reached 60% to 96% of their APMHR was 35% greater compared with those who reached their APMHR (p = 0.001). A subgroup analysis among subjects who reached 85% of their APMHR showed that even mildly attenuated heart response (in the range of 85% to 96% APMHR) was independently associated with 36% increase in CVD risk (p <0.001). In conclusion, attenuated HR response during exercise is a powerful and independent predictor of adverse cardiovascular events during long-term follow-up among healthy men and women. The prognostic implications of attenuated HR response in this population are apparent even with a minor decrease of the maximal HR to <96% of the APMHR.
Attenuated maximal heart rate (HR) during maximal exercise, termed chronotropic incompetence, is a strong predictor of cardiovascular morbidity and mortality. It is independent of other confounding factors, including ST-segment changes during exercise or coronary artery disease. Chronotropic incompetence predicts adverse cardiovascular outcomes among different populations, including healthy men and women, patients with known coronary artery disease, and patients with heart failure. Chronotropic incompetence lacks standard definition, with most studies using 85% of the age-predicted maximal HR (APMHR) as the acceptable threshold. Some definitions of chronotropic incompetence require other parameters in addition to the maximal HR, including HR at rest or METs at different stages of the exercise. The exact threshold below which healthy subjects can be considered to have increased risk for adverse cardiovascular events during long-term follow-up is not known. Therefore, the aims of the present study were to (1) describe the association between the HR response during exercise and subsequent cardiovascular morbidity in a large cohort of asymptomatic men and women free of diabetes or ischemic heart disease and (2) identify the degree of chronotropic incompetence associated with long-term adverse cardiovascular events in this population.
Methods
The Institute for Preventive Medicine of the Chaim Sheba Medical Center performs approximately 9,000 annual screening examinations. All participants are interviewed at the time of each annual examination using standard questionnaires that gather information about demographic characteristics, medical history, and health-related habits. Thereafter, blood samples are drawn after a 12-hour fast and analyzed immediately. A physician at the center performs a complete physical examination, including blood pressure measurement. All subjects undergo a standard exercise stress test each year and are instructed not to take β blockers in the morning of their visit. A computerized database of all the annual examinations performed in this center was established in the year 2000 and is the source of data for the study. The Institutional Review Board of the Sheba Medical Center approved this study on the basis of strict maintenance of participants’ anonymity during database analyses. Data from subjects were recorded anonymously. No individual consent was obtained.
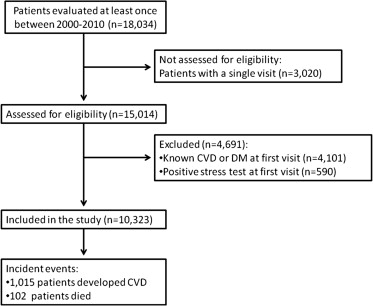
The study population comprised Caucasian men and women >34 years of age, free of ischemic heart, cerebrovascular diseases, or diabetes mellitus and with plasma fasting glucose <126 mg/dl. Subjects with pathologic, abnormal, or inconclusive exercise stress test in their first visit were excluded. Additionally, follow-up data must have been available from at least 1 subsequent visit (average number of visits per subject, 5; range, 2 to 9). A total of 18,034 subjects with available data were included in the database. The final study sample comprised 10,323 subjects ( Figure 1 ). Baseline characteristics, cardiovascular risk factors, and HR response of the 3,020 subjects who had a single visit were not statistically different from the characteristics of the included subjects (data not shown).
At each annual visit, each participant had a treadmill exercise test according to the Bruce protocol in the presence of a board-certified cardiologist. Participants were instructed not to take β blockers in the morning of the visit. APMHR was defined as (220−age) for all subjects. Maximal HR was defined as the maximal HR during the stress test, as documented by the cardiologist during the test. HR response was defined as the maximal HR in beats/min divided by the APMHR and is presented in percentage in all statistical analyses. Study population was divided into 3 prespecified tertiles based on the percent APMHR reached at the baseline stress test (60.5% to 96.5%, 96.6% to 98.8%, and 98.9% to 130.6% of APMHR).
Diagnosis of cardiovascular disease (CVD) was the primary end point of the study. The outcome was defined as significant coronary heart disease (angiographically proved stenosis of >50% in at least 1 coronary artery), myocardial infarction, or acute coronary syndrome reported at the yearly visit and approved by the attending physician as well as cerebrovascular disease (see later). All-cause mortality was defined as a secondary end point of the study. Cerebrovascular outcome included cerebrovascular events or transient ischemic attacks, which were diagnosed based on a clinically significant neurologic deficit, self-reported, or based on the participants’ medical record and approved by the attending physician.
End points for termination of the exercise test were clinically significant ST-segment depression (>2 mm depression in 2 contiguous leads measured 80 ms after the J point), intolerable symptoms of angina, and exhaustion or achievement of the APMHR without such findings. All cases with a pathologic stress test were referred for coronary angiography. In participants with a borderline stress test or when participants reported angina symptoms without diagnostic electrocardiographic changes, stress perfusion imaging with thallium-201 was performed. Those with a pathologic thallium-201 cardiac scan underwent coronary angiography. For subjects with a positive stress test for whom data on coronary angiography or thallium-201 cardiac scan were not available, a positive stress test was considered as confirmation for a positive coronary heart disease.
Baseline clinical characteristics by percent APMHR tertiles were compared by either using 1-way analysis of variance for continuous variables or chi-square test for categorical variables to calculate the statistical significance of the independent variables’ trend of means across HR response tertiles. The probability of the development of a first CVD event during follow-up was estimated and graphically displayed according to the method of Kaplan and Meier, with comparison of cumulative events across strata by the log-rank test. Multivariate Cox proportional hazards regression modeling was carried out to evaluate baseline factors independently associated with the development of the composite CVD outcome. Prespecified covariates in the multivariate models included HR response (categorized to 3 tertiles), age (continuous), gender, systolic blood pressure (continuous), low-density lipoprotein cholesterol (continuous), current smoking status (yes or no), obesity (body mass index >30 or ≤30 kg/m 2 ), regular physical activity (yes or no), family history of coronary disease (yes or no), the use of β blockers, the total number of cardioprotective medication groups used out of 5 predefined groups (antiplatelets, inhibitors of the renin-angiotensin axis, diuretics, rate-control, and lipid-lowering drugs), HR at rest (continuous), HR recovery (continuous), the level of activity during the exercise (categorized into 3 tertiles) and the cardiologists’ final conclusion of the exercise stress test (normal, inconclusive, or suspected of ischemia). All statistical analyses were performed with SPSS (version 20.0) statistical software (IBM Corporation, Armonk, New York).
Results
Data of 10,323 men and women free of diabetes or CVD were analyzed in this study. The study population included 7,579 men (73%) and 2,744 women (27%). Mean age was 50.4 ± 9.2 years, mean body mass index was 26.1 ± 3.7 kg/m 2 , and mean low-density lipoprotein cholesterol was 125.6 ± 28.3 mg/dl. A total of 13.5% of the study population had hypertension and 16% were active smokers ( Table 1 ).
| Characteristic ∗ | All | First Tertile, n = 3,452 (60.5%–96.5%) | Second Tertile, n = 3,462 (96.6%–98.8%) | Third Tertile, n = 3,409 (98.9%–130.6%) |
|---|---|---|---|---|
| HR response (%) † | 95.7 ± 5.9 | 90.5 ± 6.5 | 98.2 ± 0.93 | 102.0 ± 2.4 |
| Age (yrs) † | 50 ± 9 | 52 ± 10 | 49 ± 8 | 50 ± 8 |
| Men † | 73 | 67 | 76 | 78 |
| Body mass index (kg/m 2 ) † | 26 ± 4 | 27 ± 4 | 26 ± 3 | 25 ± 4 |
| Systolic blood pressure (mm Hg) † | 120 ± 20 | 122 ± 22 | 121 ± 19 | 117 ± 18 |
| HR at rest (beats/min) † | 76 ± 16 | 73 ± 16 | 77 ± 16 | 79 ± 17 |
| Low-density lipoprotein cholesterol (mg/dl) † | 126 ± 28 | 125 ± 28 | 127 ± 28 | 124 ± 28 |
| Hypertension † | 14 | 21 | 11 | 8 |
| Current smoker † | 16 | 20 | 14 | 13 |
| Physical activity | 63 | 61 | 62 | 64 |
| Family history of ischemic heart disease | 33 | 33 | 32 | 32 |
∗ All values are reported as percentages or means ± SD.
Maximal HR during the baseline exercise stress test was documented in all 10,323 subjects. Five hundred seven subjects (5%) failed to achieve 85% of the APMHR (mean HR response was 95.7 ± 6.0%). The baseline clinical characteristics of study patients by tertiles of percent APMHR reached at the baseline stress test are presented in Table 1 . Average HR response was 90.5 ± 6.5% in the first tertile, 98.2 ± 0.93% in the second tertile, and 102 ± 2.4% in the third tertile. Mean age was greater in the first HR response tertile and similar in the upper 2 tertiles. The frequency of men increased with increasing tertiles of HR response, whereas mean body mass index, the frequency of hypertension and of smokers were all inversely correlated with increasing tertiles of percent APMHR reached ( Table 1 ).
During 44,806 person-years of follow-up (mean follow-up of 4.3 years), there were 1,015 (9.8%) documented incident cases of CVD end points (936 cases of coronary artery disease, 79 cases of cerebrovascular events). One hundred two subjects died during the follow-up period (1%).
Compared with the upper tertile (98.9% to 130.6% of APMHR), patients in the lowest tertile (60.5% to 96.5% of APMHR) had a significant 61% (p <0.001) increase in the unadjusted risk for the development of CVD outcomes during follow-up and patients in the middle tertile had a corresponding 24% (p = 0.02) risk increase ( Table 2 ). Consistent with those findings, Kaplan-Meier survival analysis showed that the cumulative probabilities for the development of CVD at 4-year follow-up were 6.6% among subjects in the upper HR response tertile, 8.5% among those in the middle tertile, and 10.4% among those in the lowest tertile (log-rank p value <0.001 for the overall difference during follow-up; Figure 2 ).
| Event | Unadjusted Hazard Ratio (95% CI) | Number of Events | ||||
|---|---|---|---|---|---|---|
| Lower Tertile | Middle Tertile | Upper Tertile (Reference) | Lower Tertile | Middle Tertile | Upper Tertile | |
| Cardiovascular or cerebrovascular disease | 1.61 (1.38–1.86) | 1.24 (1.06–1.46) | 1 | 428 | 338 | 249 |
| CVD | 1.53 (1.30–1.80) | 1.22 (1.03–1.45) | 1 | 385 | 315 | 236 |
| Cerebrovascular disease | 3.09 (1.66–5.75) | 1.58 (0.81–3.14) | 1 | 43 | 23 | 13 |
| All-cause mortality | 1.72 (1.03–2.86) | 0.95 (0.54–1.66) | 1 | 50 | 30 | 22 |
The fully adjusted multivariate model showed that compared with the upper tertile of HR response, the lower tertile was independently associated with a significant 35% (p = 0.001) increased hazard ratio for the development of CVD during follow-up and the middle tertile was associated with a corresponding 23% (p = 0.01) increase of hazard ratio ( Table 3 ). Additional factors in the multivariate model independently associated with increased hazard ratio for CVD events were gender, age, low-density lipoprotein cholesterol, systolic blood pressure at rest, regular physical activity, family history of CVD, the use of cardioprotective drugs, and the cardiologist’s final conclusion of the exercise stress test. Notably, HR recovery during the index exercise test was not shown to be significantly associated with outcome after adjustment for HR response, suggesting that the latter measure may have more important prognostic implications.
| Variable | Hazard Ratio | 95% Confidence Interval | p Value | p Value for Interaction ∗ |
|---|---|---|---|---|
| HR response | ||||
| Upper tertile | 1 | |||
| Middle tertile | 1.23 | 1.04–1.45 | 0.01 | |
| Lower tertile | 1.35 | 1.14–1.6 | 0.001 | |
| Age (1-yr increment) | 1.05 | 1.04–1.56 | <0.001 | 0.51 |
| Men | 1.74 | 1.47–2.06 | <0.001 | 0.33 |
| Current smoking | 1.13 | 0.95–1.34 | 0.16 | 0.60 |
| Body mass index ≤30 kg/m 2 | 0.87 | 0.72–1.06 | 0.16 | 0.86 |
| Low-density lipoprotein cholesterol (1 mg/dl increment) | 1.004 | 1.002–1.006 | 0.001 | 0.60 |
| SBP (1-mm Hg increment) | 1.005 | 1.001–1.008 | 0.007 | 0.48 |
| Regular physical activity | 0.38 | 0.33–0.46 | <0.001 | 0.03 |
| Family history of ischemic heart disease | 1.25 | 1.10–1.42 | 0.001 | 0.05 |
| β Blockers | 1.27 | 0.97–1.66 | 0.09 | 0.43 |
| HR at rest (1 beat/min increment) | 0.997 | 0.993–1.002 | 0.24 | 0.59 |
| HR during recovery (1 beat/min increment) | 1.000 | 0.997–1.004 | 0.85 | 0.1 |
| Cardioprotective drugs | ||||
| None | 1 | |||
| 1 | 0.71 | 0.59–0.85 | 0.003 | 0.36 |
| 2 | 0.65 | 0.52–0.82 | 0.002 | 0.18 |
| 3 | 0.53 | 0.37–0.75 | 0.003 | 0.71 |
| 4 | 0.10 | 0.04–0.28 | <0.001 | 0.53 |
| 5 | 0.08 | 0.01–0.56 | .014 | 0.98 |
| METs (kcal·kg −1 h −1 ) | ||||
| 1.1–10.1 | 1 | |||
| 10.2–12.9 | 0.84 | 0.71–0.98 | 0.030 | 0.25 |
| >13 | 0.82 | 0.64–1.06 | 0.125 | 0.43 |
| Missing data | 0.88 | 0.74–1.04 | 0.131 | 0.46 |
| Ergometry results | ||||
| Normal | 1 | |||
| Inconclusive | 2.688 | 2.19–3.30 | <0.001 | 0.06 |
| Suspected | 5.330 | 3.23–8.79 | <0.001 | 0.67 |
| Missing | 2.744 | 2.37–3.19 | <0.001 | 0.37 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


