Figure 15.1
Transesophageal echo (mid-esophageal view) showing ascending aortic aneurysm (7.28 cm)
Acute aortic dissection starts with a tear in the aortic intima following which blood enters the tear separating the intima from the media or adventitia, creating a false lumen. Propagation depends on BP and the pulse wave (rate of change in pressure/time) whereby high blood pressure and rapid ventricular contractions abet further migration. Complications such as malperfusion syndromes, tamponade, or aortic valve insufficiency are responsible for the subsequent clinical picture.
Two different anatomic systems, the DeBakey and Stanford systems, are used to classify aortic dissection [1, 2].
Aortic dissection is confirmed when 2 lumens are separated by an intimal flap visualized within the aorta. Tears can be identified and differentiation between true and false lumen is often easy and diagnostic with optional color Doppler flow mapping; intimal tear(s) can be localized in the majority of patients (Fig. 15.2).
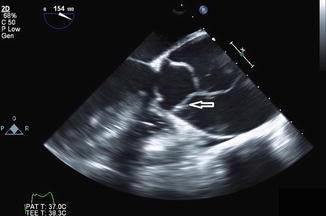
Figure 15.2
Transesophageal image showing an aortic dissection intimal flap (arrow) inside true wall
Transoesophageal echocardiography is the echocardiographic imaging method of choice as it provides excellent visualization of ascending aorta, descending thoracic aorta and mechanism of aortic insufficiency. TEE is limited in assessing abdominal side branches and may be unpleasant for patients who cannot tolerate topical anesthesia and moderate conscious sedation.
Transthoracic echo (TTE) can be performed as an initial test for evaluation of aortic dissection if patient is very unstable and other modalities of imaging are not readily available. It can be performed at the bedside and can reveal acute aortic regurgitation and presence of an intimal flap (Fig. 15.3), although image resolution is not as good as TEE in general. It usually provides adequate visualization of aortic root and early part of ascending aorta. Suprasternal and subcostal windows can provide limited but valuable data regarding aortic arch and descending aorta respectively.

Figure 15.3
Transthorasic echo view of thrombosed false lumen of descending aortic dissection (arrow)
Aortic Intramural Hematoma
Aortic intramural hematoma (IMH) is a variant of aortic dissection and is classified similarly. It is differentiated from aortic dissection by the absence of a detectable intimal tear and hence and hence, absence of continuous flow communication (Fig. 15.4).
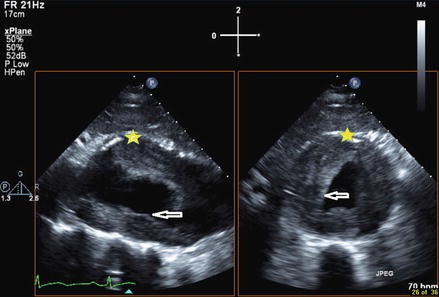




Figure 15.4
Biplane view of mural thrombus (arrows) inside abdominal aorta (star)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
