Diagnostic Thoracic Surgical Procedures: Thoracoscopy, VATS, and Thoracotomy
INTRODUCTION
Thoracoscopy, video-assisted thoracic surgery (VATS), and thoracotomy are well-established surgical techniques used by thoracic surgeons to diagnose benign and malignant diseases involving the thorax.
Thoracoscopy first emerged as a diagnostic tool in the early 20th century when therapeutic pneumothorax became the surgical treatment of choice for tuberculosis. In 1910, Hans Christian Jacobaeus performed the first thoracoscopic intrapleural pneumolysis for collapse therapy in the treatment of tuberculosis.1–3 He used a rigid cystoscope with a light source to access the pleural cavity and perform a pneumolysis. After development of effective antimicrobial therapy for tuberculosis, thoracoscopy evolved as an effective diagnostic procedure to evaluate pleural effusions and pleural disease.4 During direct diagnostic thoracoscopy, a fiberoptic mediastinoscope or bronchoscope was placed through a small intercostal incision; pleural fluid could be aspirated and sent for analysis (Fig. 37-1). In addition, the parietal pleura, visceral pleura, fissures, hilum, and diaphragm could be inspected directly.5
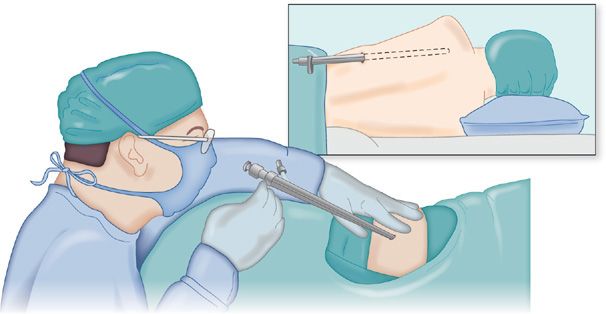
Figure 37-1 Use of a rigid bronchoscope as a thoracoscope.
By 1990, thoracoscopy evolved into VATS. Development of high-resolution video cameras and endoscopic linear mechanical stapling devices allowed the expansion of application of VATS into the diagnosis and treatment of pulmonary nodules and interstitial lung diseases (ILDs).6,7 The use of diagnostic thoracotomy has declined significantly since the emergence of VATS; however, the diagnostic thoracotomy may be necessary in cases in which VATS is not feasible (Table 37-1).
TECHNICAL CONSIDERATIONS
VATS is performed in the operating room under general anesthesia. A double-lumen tube is placed to isolate the lungs to enable establishment of one-lung ventilation, which is essential for performing the procedure. The use of one-lung ventilation creates sufficient space for maneuvering within the hemithorax to perform the planned procedure. Carbon dioxide (CO2) insufflation can also be used to provide additional working space within the chest cavity by lowering the position of the diaphragm. The more inferiorly located diaphragm provides better exposure of the costophrenic sulci and lower lobes. When CO2 is used, the maximum insufflation pressure is maintained below 6 mm Hg to avoid decreased venous return to the right heart and associated hypotension.
The typical VATS procedure utilizes three to four incisions that range from 5 to 12 mm in size. The incisions are usually arranged in a triangular configuration, with the area of interest located in the center of the triangle. (Fig. 37-2) A 5- or 10-mm fiberoptic thoracoscope is connected to a video camera and is most commonly inserted into the most inferiorly placed VATS incision (Fig. 37-3). The chest cavity is clearly visualized on a video monitor and the parietal pleura, visceral pleura, hilum, diaphragm, and mediastinum can be directly inspected. Upon completion of the procedure, a chest tube is inserted under direct visualization through one of the VATS incisions to evacuate air and pleural fluid during the early postoperative period. Simple diagnostic VATS procedures are typically well tolerated, and patients can be discharged after 1 to 2 days in the hospital. Currently, the disease processes assessed using VATS are listed in Table 37-2.
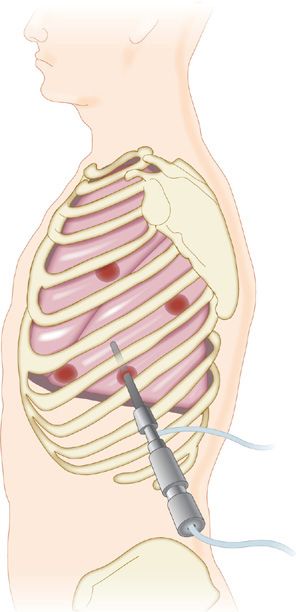
Figure 37-2 Placement of VATS incisions.
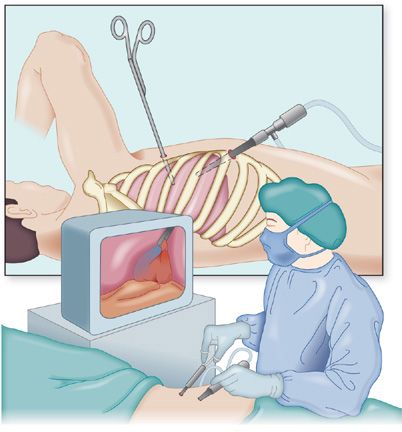
Figure 37-3 Placement of the thoracoscope through the most inferior of the VATS incisions. A video camera is connected to the thoracoscope and the image displayed on a video monitor.



