Ever since the publication of the East-West Study, diabetes mellitus has been considered a coronary heart disease equivalent. This position has been accepted by the National Cholesterol Education Program. The question that must be asked, however, is this: Is it the entity of diabetes as a whole that is causal of coronary heart disease, or is it a component or components of the diabetes constellation that are causal?
The report by Rasmussen-Torvik et al shows that the risk for atherothrombotic disease (ATD) of the heart is attenuated by high-density lipoprotein cholesterol and that ATD of the brain is attenuated by hypertension, at least that portion of ATD risk attributed to diabetes, as measured by fasting insulin levels. This is important because it means that the link between diabetes and ATD is related to dyslipidemic hypertension. This finding is supported by the finding in 3 major trials that tight control of blood sugar levels (BSLs) does not favorably affect cardiovascular mortality: Action to Control Cardiovascular Risk in Diabetes (ACCORD), Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE), and the Veterans Affairs Diabetes Trial (VADT). Indeed, in ACCORD, ATD mortality was higher in the tight-control group.
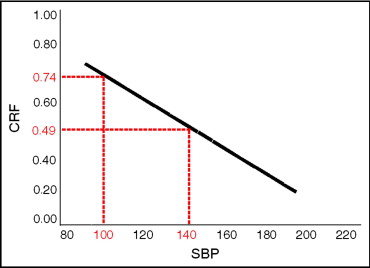
I can extend the findings of the Atherosclerosis Risk in Communities (ARIC) study. I presented data at the 2009 symposium of the International Atherosclerosis Society in Boston, and again at the 2010 symposium of the National Lipid Association, showing that knowledge of the 2-hour postprandial BSL is irrelevant to the prediction of the population at risk for ATD. The National Lipid Association presentation is published in abstract form. The data will be presented again at the 2010 symposium of the European Atherosclerosis Society in Hamburg, Germany, in June. The prediction of the population at risk for ATD is highly accurate when the Bowling Green Study (BGS) graph is used ( Figure 1 ). The BGS graph has been presented in The American Journal of Cardiology and has been published in full elsewhere. The validation of the BGS graph was presented at the 2010 National Lipid Association symposium. The BGS graph has a lipid arm (combining low-density lipoprotein and high-density lipoprotein into a ratio called the cholesterol retention fraction [CRF] and defined as [low-density lipoprotein − high-density lipoprotein]/low-density lipoprotein) and a blood pressure arm (using systolic blood pressure [SBP]). The ATD threshold line has coordinates (0.74, 100) and (0.49, 140). Eighty-five percent of all patients with ATD in the author’s database have CRF-SBP plots above the threshold line, and of the 15% of patients with ATD with CRF-SBP plots below the threshold line, most are cigarette smokers, leaving only 6% of the ATD population that cannot be predicted by CRF-SBP plot position above the threshold line and/or cigarette smoking status. The predictions of the population at risk for ATD are the same whether the 2-hour postprandial BSL is ≤99 mg/dl or ≥200 mg/dl—and anywhere in between. Indeed, the predictions are the same even if the physician has no knowledge of the 2-hour postprandial BSL.