Fig. 16.2 This ECG shows the classic ‘proximal LAD’ pattern. The patient is in sinus rhythm. There are good (probably normal sized) R waves throughout the ECG (i.e. there has been no previous myocardial infarction). Antero-laterally (i.e. leads I, II, aVL and V2–6) there is deep symmetrical T wave inversion (i.e. the downslope is the same configuration as the upslope, unlike ‘reverse-tick’ T wave inversion). This pattern is almost pathognomonic of a high-grade acute (i.e. thrombotic) lesion in the proximal portion of the left anterior descending coronary artery, requiring early revascularization. There are several much rarer causes of this ECG (see text).
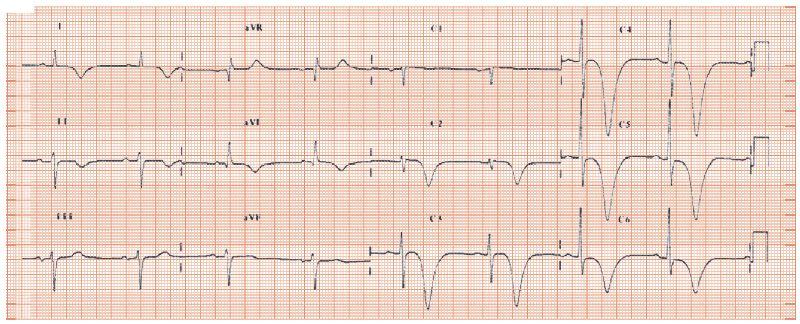
Fig. 16.3 T wave inversion in left bundle branch block (LBBB). This ECG shows sinus rhythm, normal PR interval, and a broad QRS complex, with the morphology of LBBB. The lateral leads (I, II, aVL, V5, V6) show abnormal repolarization; whether this is called ST depression, or T wave inversion is semantic. It is universal in LBBB, and indicates that the direction of the repolarizing current is reversed.
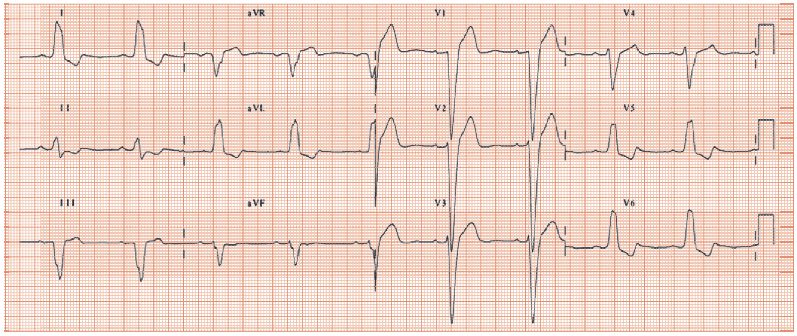
Fig. 16.4 ECG with digoxin effect. Sinus rhythm, long PR interval (280 ms), due to digoxin’s vagal enhancing effect. Normal QRS complexes. ‘Reverse-tick’ T wave. Digoxin increases the chance of ST depression occurring during an exercise test, regardless of whether or not coronary disease is present.

Major T wave inversion is important as it often indicates a major illness.
ECG features of T wave inversion
The normal T waves follow the polarity of the R wave: in health leads with large R waves have upright T’s, leads with equivocal R waves have flat T waves, and leads with deep S waves have inverted T’s. T wave inversion can only be diagnosed when it occurs in a lead with a large R wave where an upright T wave is expected. If the R wave should be large, but isn’t due to disease, then T wave changes are secondary to the process that has affected the R wave. T wave abnormalities include T wave flattening/mild inversion (see Chapter 15); major T wave inversion is discussed here.
Morphology of T wave inversion
- The inverted T wave may be symmetrical, with the down slope and upslope having the same angle, common in coronary disease (Figs 16.1 & 16.2).
- Asymmetrical T wave inversion: the down slope is much shallower than the upslope, resulting in a ‘reverse-tick’ appearance. Common in left ventricular hypertrophy (LVH), bundle branch block (BBB) (Fig. 16.3), coronary disease and digoxin (Fig. 16.4).
- Biphasic T waves, with the first part going up, and the second part down. This is common in acute coronary syndrome and following a myocardial infarction.
- Biphasic T waves, with the first part going down, and the second part up. This pattern is common in coronary disease in the few minutes after exercise, reported as ‘following exercise typical ischaemic repolarization changes occurred.’ Its presence increases the probability of coronary disease.
Causes of deep T wave inversion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


