Congenitally corrected transposition of the great arteries (CCTGA) is an uncommon cardiac anomaly. It is characterized by atrioventricular (AV) and ventriculoarterial (VA) discordance (Fig. 10.1). The discordance of both the AV and VA connections results in a situation where the systemic and pulmonary venous returns are appropriately directed to the pulmonary artery and aorta. However, the arrangement of the morphologic ventricles “between” the venous and arterial segments is the opposite of normal. The systemic venous return connects with the right atrium (RA) normally. The RA is then connected to the morphologic left ventricle (LV) via a mitral valve that is in turn connected to the pulmonary artery (PA). There is no subpulmonary infundibulum because this is a morphologic LV and therefore there is mitral valve–pulmonary valve fibrous continuity. The pulmonary veins connect to the left atrium (LA). The LA is then connected to a morphologic right ventricle (RV) via a tricuspid valve. The RV (systemic ventricle) is connected to the aorta. In CCTGA, the aorta is usually positioned anterior and leftward of the pulmonary artery with a well-developed subaortic infundibulum resulting in discontinuity between the tricuspid and aortic valves.
CCTGA is often referred to as “l” (levo)-transposition of the great arteries. This “l” refers to the leftward embryologic looping of the ventricles and not the spatial relationship of the great arteries. It is a confusing term given that many other complex conditions, including forms of single ventricle, can have l-transposed (anterior and leftward) great arteries. Simply referring to CCTGA as “corrected transposition” is also inadequate since patients with complete or d (dextro)–TGA may have been “surgically corrected.” For these reasons, the authors prefer the term “congenitally corrected transposition of the great arteries (CCTGA)” to describe patients with AV and VA discordance.
ECHOCARDIOGRAPHIC ASSESSMENT
Echocardiography is the imaging modality that provides the most robust diagnostic assessment of CCTGA. The unusual relationship between the two ventricles, ventricular septum, and the great arteries results in several unique echocardiographic features. Similar to other forms of transposition of the great arteries, the initial (unbranched) segments of the great arteries run parallel to each other (Fig. 10.2). In addition, unlike the normal heart, the ventricles assume more of a side-by-side relationship, and as result, the ventricular septum is oriented in a straight anterior–posterior plane (Fig. 10.3). In some cases, the ventricles are arranged in a superior-inferior manner with the morphologic RV being superior. The diagnosis of CCTGA is based on demonstrating discordance of both the AV and VA connections [RA → LV → PA, and LA → RV → aorta]. The spatial relationship of the great arteries supports the diagnosis of CCTGA; however, it should not be considered the sole diagnostic criterion.
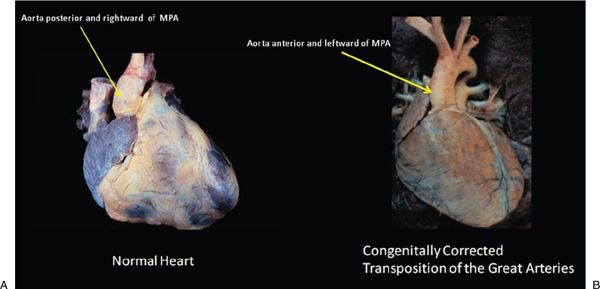
Figure 10.1. Pathology specimen. A: Normal relationship of great arteries to the ventricles (ventriculoatrial [VA] concordance) and normally related atrioventricular (AV) relationships (AV concordance). B: Congenitally corrected transposition of the great arteries with AV discordance and VA discordance. Aorta is anterior and leftward to main pulmonary artery. (From the Dr. William Edwards collection, Mayo Clinic.)

Figure 10.2. Subcostal imaging with transducer angulated anterior to demonstrate parallel relationship of the great arteries.
The subcostal and apical four-chamber imaging planes are extremely useful in the examination of patients with CCTGA. The subcostal plane is used to define the atrial and visceral situs and the cardiac position. Twenty-five percent of patients with CCTGA have dextrocardia or mesocardia (Fig. 10.4). The subcostal views allow excellent imaging of the great arteries and their relationships to the ventricular chambers. From the subcostal coronal imaging plane, the parallel arrangement of the great arteries can be easily identified (see Fig. 10.2). In addition, the unique relationship of the LV outflow tract and the PA can be seen with pulmonary outflow tract deeply wedged between the right and left AV valves (Fig. 10.5). Most importantly, in this imaging plane, the relationship of the atria, ventricles, and the great arteries can be defined. As described in previous chapters in this textbook, a morphologic RV can be defined by the presence of several unique anatomic features:
1.apical position of the tricuspid valve septal leaflet hinge point (relative to the mitral valve anterior leaflet septal hinge point),
2.a “tricuspid” trileaflet AV valve with chordal attachments to the ventricular septum,
3.a moderator band,
4.an irregular (trabeculated) mural endocardial surface,
5.a pyramidal (instead of elliptical) shape to the ventricular cavity (see Fig. 10.3).
In the most common form of CCTGA (Fig. 10.6), the pulmonary veins will connect to the left-sided LA. The LA in turn connects to a morphologic RV via a tricuspid valve. The RV then connects to a great artery that arches and gives rise to coronary arteries, and is by definition the aorta. On the other side of the heart, the systemic veins connect to a right-sided RA, which then connects to a morphologic LV. The LV connects to a great artery that bifurcates into two branches, and is by definition the pulmonary artery. In the young patient, these connections and relationships can be observed from the subcostal transducer position.
Similar to the subcostal coronal imaging plane, the apical four-chamber plane is extremely useful in the setting of CCTGA. In fact, the key anatomic feature of AV discordance is best visualized in the four-chamber plane. In this imaging plane, the septal hinge points of the AV valves are readily appreciated (see Fig. 10.3). In situs solitus of the atria and concordant AV connections, the AV valve associated with the RA and RV will have a septal hinge that is displaced toward the apex when compared to the contralateral valve. In situs solitus of the atria and CCTGA, due to the discordant AV connection, it is the left-sided AV valve hinge point that is closer to the ventricular apex. Additional scans from the apical transducer position can define the anatomy of the AV valves, ventricular morphology, discordant AV connection, and the VA relationships (Fig. 10.7A). In addition, AV valve abnormalities, LV outflow tract obstruction (Fig. 10.7B) and muscular ventricular septal defects (VSDs) can be evaluated.
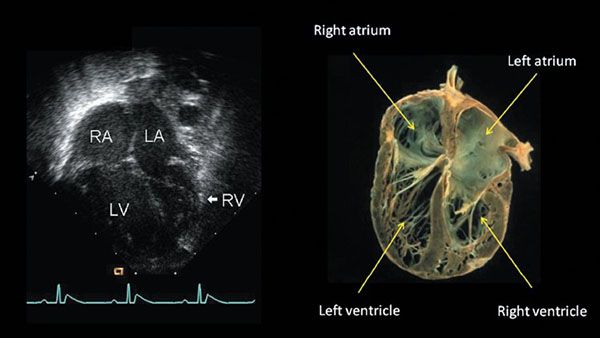
Figure 10.3. Apical four-chamber view demonstrating anterior–posterior relationship of ventricular septum resulting in a more vertical orientation of the septum and side-by-side relationship of ventricles. Left-sided ventricle is the morphologic right ventricle and right-sided ventricle is the morphologic left ventricle.
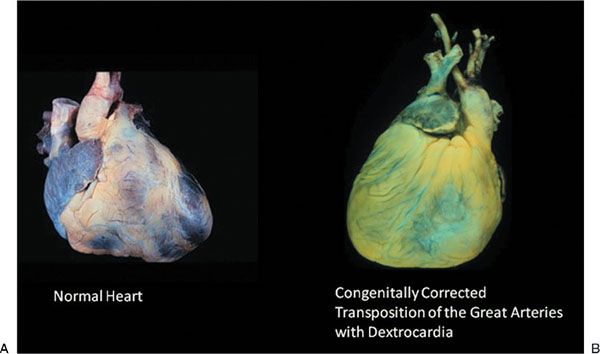
Figure 10.4. Pathology specimens. A: Levocardia with normally related great vessels (ventriculoatrial [VA] concordance) and atrioventricular (AV) concordance. B: Congenially corrected transposition of the great arteries with dextrocardia. (From the Dr. William Edwards collection, Mayo Clinic.)
Apical four-chamber imaging is more challenging when the ventricles are positioned in a superior and inferior fashion. In these patients it will not be possible to image both AV valves in the same plane. In this setting, the transducer will need to be tilted inferiorly to see the right-sided mitral valve and superiorly to see the left-sided tricuspid valve. The septal hinge point relationship is more difficult to appreciate. The diagnosis of CCTGA in these patients relies on the other features which define ventricular morphology.

Figure 10.5. Subcostal imaging plane with transducer angulated anterior and superior. Demonstrates the unique anatomy of the left ventricle in CCTGA with the pulmonary outflow tract (arrow) deeply wedged between the right and left atrioventricular valves.
The side-by-side relationship of the ventricles, more vertical orientation of the ventricular septum, and side-by-side relationship of the great arteries all make the parasternal long-axis views in CCTGA confusing. Unlike in the normal heart, the long axis in CCTGA is more vertically oriented (Fig. 10.8). This allows easy confirmation of the parallel arrangement of the great arteries. However, because of the side-by-side relationship of the ventricles, when the transducer is placed in a standard long-axis imaging position, several views are obtained, including a long-axis image through the LV and pulmonary artery (see Fig. 10.8A) and a long-axis image through the morphologic RV and aorta (see Fig. 10.8B). Adding to the confusion, from the same standard long-axis imaging plane, it is also possible to obtain an image through the pulmonary valve and the left AV valve. The membranous septum is thin and often shifted to the right, away from this imaging plane. As a result, this plane can give the false impression that the left AV valve and the posteriorly positioned pulmonary valve are related to the same (left-sided) ventricle. A large ventricular septal defect (VSD) may make this plane of imaging even more challenging. In this setting, the pulmonary valve appears related to both AV valves, creating the appearance of a single ventricle. Nevertheless, the long-axis imaging plane is useful for evaluating the great artery relationships and for detecting the presence of outflow tract obstruction.
The short-axis imaging plane in the setting of CCTGA is also very helpful. The ventricular septum in CCTGA is more horizontally oriented than it is in the normal heart (Fig. 10.9A). At the level of the aortic and pulmonary valves, the relationship of the great arteries can be confirmed. In the majority of cases, the aortic valve will be leftward, anterior, and superior to the pulmonary valve (Fig. 10.9B). With slight superior angulation from the level of the aortic valve, the coronary arteries can be identified (Fig. 10.9C). In 85% of cases, the coronary arteries will be inverted. The coronary artery that arises from the left posterior–facing sinus has the epicardial distribution of a morphologic right coronary artery. Conversely, the coronary artery arising from right posterior–facing sinus has the epicardial distribution of a morphologic left coronary artery and gives rise to an anterior descending branch and a right-sided posterior “circumflex” branch. A single coronary artery is the most common coronary anomaly in CCTGA. With further superior angulation of the transducer, the bifurcation of the PA can be identified. This image confirms the posterior position of the PA (Fig. 10.9D).
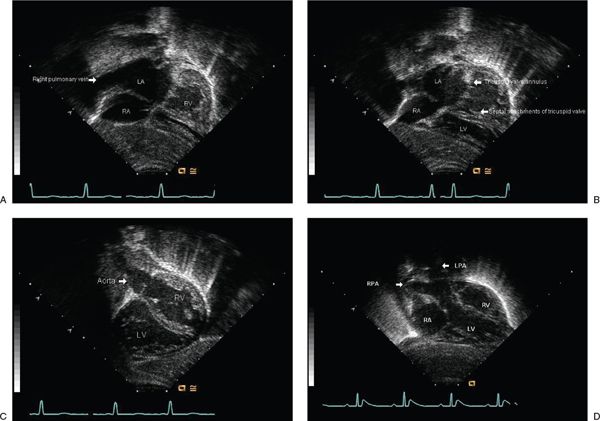
Figure 10.6. Subcostal imaging in CCTGA. A: Subcostal coronal image demonstrating the most common form of congenitally corrected transposition of the great arteries (TGA) with the pulmonary veins connected to the left-sided atrium. B: Subcostal coronal imaging with transducer angulated anterior and superior demonstrating that the left atrium (LA) connects to a morphologic right ventricle (RV) and the septal attachments of the left-sided morphologic tricuspid valve (arrows). C: With the transducer angulated even more superior, the relationship of this ventricle to a great artery that arches and then gives rise to coronary arteries (aorta) is identified. D: Subcostal coronal image demonstrating relationship of the right-sided structures. Right-sided atrium drains to morphologic left ventricle that then gives rise to an artery that branches (arrows), the main pulmonary artery.
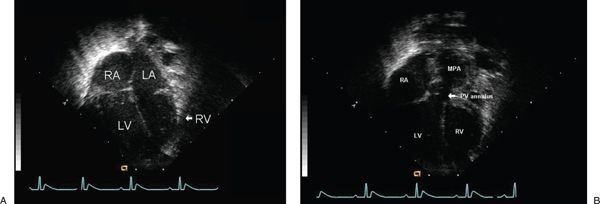
Figure 10.7. Apical inflow and outflow images of CCTGA. A: Apical four-chamber view demonstrating atrioventricular relationships in the setting of congenitally corrected transposition of the great arteries. B: Apical four-chamber image with transducer angulated anterior and superior to demonstrate the pulmonary outflow tract.
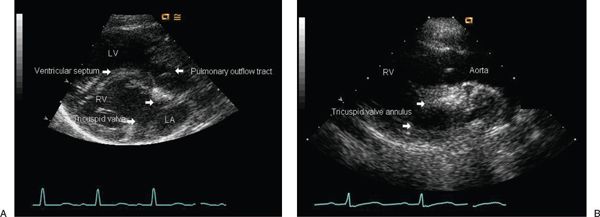
Figure 10.8. Parasternal long-axis images with transducer placed in the standard long-axis imaging position. Demonstrates the two separate long-axis views that can be obtained in congenitally corrected transposition of the great arteries with slight leftward or rightward angulation. A: Long-axis image through the morphologic left ventricle (LV) and pulmonary artery (right). B: Long-axis image through the morphologic right ventricle (RV) and aorta (left).
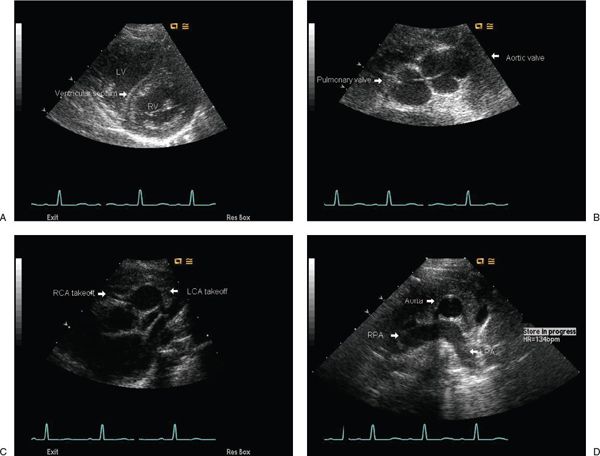
Figure 10.9. Parasternal imaging in CCTGA. A: Short-axis imaging plane demonstrating that the septum (arrow) in the setting of congenitally corrected transposition of the great arteries (CCTGA) is more horizontal than usual. B: With superior angulation of the transducer, the level of the aortic and pulmonary valves can be imaged allowing confirmation of the relationship of the great arteries (aortic valve leftward, anterior, and superior to pulmonary valve). C: With further superior angulation from the level of the aortic valve, the coronary arteries can be identified (arrows). D: With further superior angulation of the transducer, the bifurcation of the pulmonary artery can be identified confirming its posterior position.
In CCTGA, it is often difficult to image the aortic arch from the standard suprasternal position. In CCTGA, the course of the ascending aorta is straight and leftward. It then arches with the descending aorta coursing downward on the left behind the ascending aorta. As a result, to image the aortic arch and a patent ductus arteriosus in the setting of CCTGA, the transducer needs to be placed in high left parasternal position, similar to the so-called “ductal view.” In this position, it is also important to delineate the brachiocephalic branching pattern of the aortic arch given that a right aortic arch can occur in 18% of CCTGA.
ASSOCIATED CARDIAC LESIONS
Tricuspid valve abnormalities are the most common associated lesions in CCTGA, occurring in 90% of cases at autopsy. These features are best demonstrated in the apical four-chamber view but also can be seen in the subcostal coronal and modified short-axis views. The tricuspid valve is usually dysplastic, with or without displacement of the septal and posterior leaflets. Most commonly, the displacement is mild and does not meet criteria for Ebstein anomaly (Fig. 10.10). When features of Ebstein anomaly are present in CCTGA, typically the anterior leaflet is least affected, with severe involvement of both the septal and posterior leaflets. In the most severe form, there can be an unguarded tricuspid valve orifice with severe regurgitation (Fig. 10.11 A–B). When severe Ebstein anomaly is present, there can be associated RV hypoplasia with subaortic obstruction and coarctation of the aorta. This is rare, but it is always associated with an abnormal tricuspid valve with severe regurgitation and a disordered RV with marked thinning of the myocardium. Rarely, subaortic obstruction can occur with an intact ventricular septum. In these cases, the ascending aorta is usually hypoplastic. The subcostal four-chamber and short-axis imaging planes are useful for evaluating RV outflow tract obstruction. The high left parasternal view is useful for diagnosing coarctation of the aorta. Other associated left AV valve abnormalities include a supravalvular ring and varying degrees of AV valve override and straddling in the setting of a VSD.
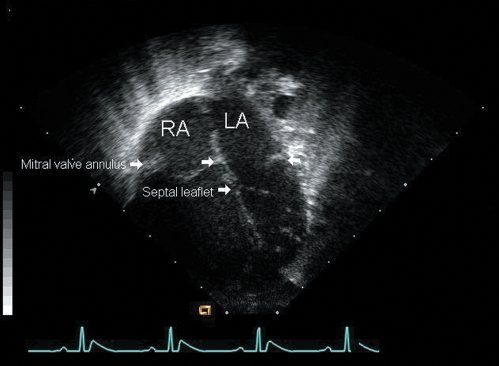
Figure 10.10. Apical four-chamber view demonstrating mild inferior displacement of the septal leaflet of the tricuspid valve (arrows
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


