Described are certain clinical and morphologic features of one patient with acute , another with subacute , and one with chronic cor pulmonale. All 3 had evidence of severe pulmonary hypertension. The patient with acute cor pulmonale 4 days after coronary bypass for unstable angina pectoris suddenly developed severe breathlessness with cyanosis and had fatal cardiac arrest and necropsy disclosed massive pulmonary embolism. The patient with subacute cor pulmonale had severe right-sided heart failure for 5 weeks and necropsy disclosed microscopic-sized neoplastic pulmonary emboli from a gastric carcinoma without parenchymal pulmonary metastases. The patient with chronic cor pulmonale had evidence of right-sided heart failure for years, the result of primary or idiopathic pulmonary hypertension almost certainly present from birth because the pattern of elastic fibers in the pulmonary trunk was that seen in newborns where the pressure in the pulmonary trunk and ascending aorta are similar. The patient with chronic cor pulmonale had plexiform pulmonary lesions indicative of irreversible pulmonary hypertension. Neither the acute nor the subacute patient had chronic pulmonary vascular changes. All 3 patients had dilated right ventricular cavities and non-dilated left ventricular cavities and only the patient with chronic cor pulmonale had right ventricular hypertrophy.
In Paul Dudley White’s third edition of his Heart Disease published in 1951, sixteen pages were devoted to acute and chronic cor pulmonale. In Braunwald’s ninth edition of Heart Disease published in 2012, cor pulmonale was not mentioned in the index, although many pages were devoted to pulmonary hypertension, the common denominator of acute, subacute, and chronic cor pulmonale. Cor pulmonale may be defined as dilatation of the right ventricular cavity without hypertrophy of its wall ( acute and subacute cor pulmonale) or both dilatation of the right ventricular cavity and hypertrophy of its wall ( chronic cor pulmonale), secondary to pulmonary hypertension not caused by a condition involving the left side of the heart. Although chronic cor pulmonale appears to have been recognized by Laennec by 1821, acute cor pulmonale was not described until 1935 by McGinn and White and the subacute form was described initially by Brill and Robertson in 1937. Although the echocardiographic or computed tomographic features of acute cor pulmonale have been well described, we were unable to find any published reports describing clinical and morphologic features in patients with all 3 forms of cor pulmonale. Our purpose herein is simply to illustrate these characteristic features in 3 patients, 1 each with the acute, the subacute, and the chronic forms of cor pulmonale.
Patient Descriptions
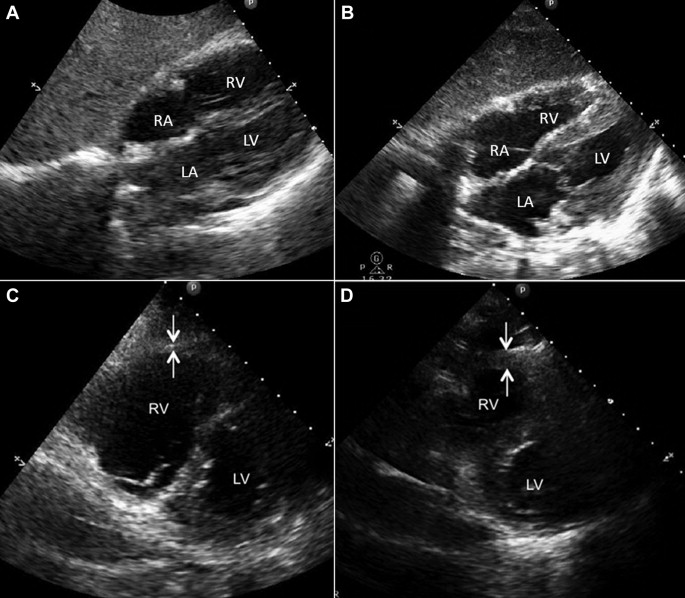
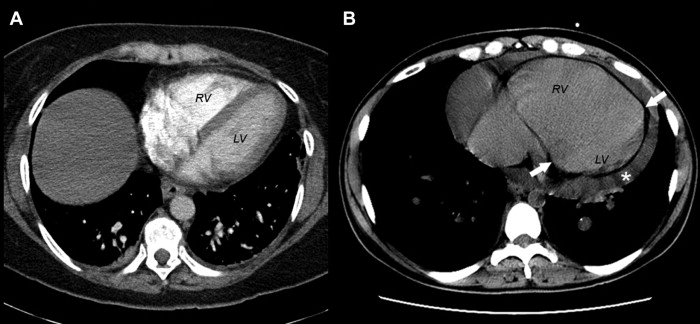
Pertinent features of each of the 3 patients are summarized in Table 1 . Echocardiographic and computed tomographic features in the subacute and chronic cases are shown in Figures 1 and 2 . The acute patient, aged 67, had symptoms suggesting a respiratory catastrophe for only several minutes and necropsy disclosed massive pulmonary emboli ( Figure 3 ); the subacute patient, aged 52, had symptoms for 5 weeks, determined at necropsy to be the result of multiple microscopic-sized pulmonary neoplastic emboli without parenchymal lung metastases from carcinoma of the stomach ( Figures 4 and 5 ), and the chronic patient, only 33 years old, had symptoms of right-sided heart failure and periodic substernal chest pain for about 20 years ( Figures 6–8 ). All 3 had very dilated right ventricular cavities, the acute and subacute patients without right ventricular wall thickening, and the chronic patient with both right ventricular dilatation and severe right ventricular wall thickening. The subacute and chronic patients had documented severely elevated right ventricular and pulmonary arterial peak systolic pressures (70 and 94 mm Hg, respectively), and the acute patient almost certainly did as well. Neither the acute nor the subacute patients had thickened walls of the pulmonary arteries and neither had plexiform lesions. The chronic patient, in contrast, had classic findings of primary pulmonary hypertension (medial and intimal thickening of the pulmonary arteries and numerous pulmonary plexiform lesions) ( Figure 8 ). Sections of the pulmonary trunk in the acute and subacute patient disclosed a typical adult pattern of the medial elastic fibers whereas in the chronic patient the pattern was that present at birth and similar to the medial elastic fiber pattern of the aorta ( Figures 9 and 10 ).
| Variable | Acute | Subacute | Chronic |
|---|---|---|---|
| Age (Years) | 67 | 52 | 33 |
| Sex | Man | Woman | Woman |
| Duration of symptoms of heart failure | < 1 hour | 5 weeks | 20 years |
| Cause of pulmonary hypertension | Massive PE | PE (Neoplastic) | PPH |
| Echocardiogram | |||
| Dilated right ventricular cavity | – ∗ | 3+/4+ | 3+/4+ |
| Dilated right atrial cavity | – ∗ | 0/4+ | 2+/4+ |
| Thickened right ventricular wall | – ∗ | 0/4+ | 4+/4+ |
| Left ventricular ejection fraction (%) | 65 | 55 | 55 |
| Pressures (mm Hg) | |||
| Pulmonary artery wedge (a/v/mean) | – | 6/10/6 | 16/18/14 † |
| Pulmonary artery (s/d) | – | 70/30 | 94/45 † |
| Right ventricle (s/d) | – | 70/14 | 94/31 † |
| Right atrium (a/v/mean) | – | 13/10/8 | 19/15/15 † |
| Systemic artery (s/d) | – | 115/70 | 90/50 |
| Cardiac index (L/min/m 2 ) | – | 1.7 | – |
| Hematocrit (%) | 43 | 37 | 41 |
| Body mass index (Kg/m 2 ) | 43 | 32 | 21 |
| Children | 1 | 3 | 0 |
| Heart and lung transplant | 0 | 0 | + |
| Heart weight (g) | 570 | 385 | 430 |
| Floating heart ‡ | + | + | + |
∗ Unable to access because of severe obesity.