Figure 9.1
Parasternal long axis (left) and apical four chamber (right) views showing epithelial lung tumor extension (arrows) in the left atrium. CT reconstruction showed direct extension of the tumor from right pulmonary vein into the left atrium
Significantly more common than primary tumors. The tumors get in the heart via bloodstream, lymphatics, direct extension and extension via vena cava or pulmonary veins.
Leukemias, melanomas, thyroid carcinomas, lung cancers, sarcomas, esophageal cancer, renal cell cancer, lymphomas, breast cancer and malignant mesotheliomas are some of the more common primary cancers [2].
Primary Cardiac Tumors
Benign Tumors
Myxoma (Fig. 9.2, Video 9.1)
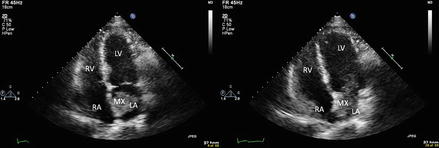
Figure 9.2
Apical four chamber view showing left atrial myxoma (MX) in systole (left) and diastole (right). Note the myxoma prolapsing through the mitral valve causing the obstruction
Most common primary cardiac tumors, up to 50 % of surgically resected primary cardiac tumors [5].
Women more commonly affected than man.
More frequently appear between 3rd and 6th decade of life.
Morphology
often pedunculated. Surface is smooth, friable or villous. Internally may contain cysts and areas of necrosis and hemorrhage.
Location
Symptoms
emboli; symptoms of mitral valve obstruction, fever, weight loss, anemia, elevated CRP [8].
Associations
Carney complex – Autosomal Dominant; multiple tumors – myxomas (presenting earlier, sometimes multiple, more likely to recur), schwannomas, endocrine tumours, blue nevi, pigmented lentigines
LAMB – lentigines, atrial myxomas, mucocutaneous myxomas, blue nevi
NAME – nevi, atrial myxomas, myxoid neurofibomas, ephelides
Imaging
Echo: Evaluate location, size, mobility, possible valvular obstruction
CT or MRI (increased intensity on T2 weighted images) – usually not needed. May help with location of attachment if not readily seen by echo.
Treatment
surgical resection
Papillary Fibroelastoma (Fig. 9.3, Video 9.2)
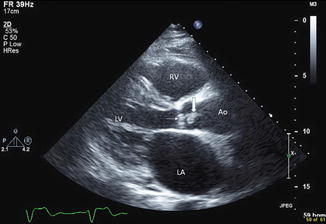
Figure 9.3
Parasternal long axis view showing Papillary Fibroelastoma (thick arrow) attached to the aortic valve (thin arrow)
Second most common primary cardiac tumors [9].
Men are more commonly affected.
Morphology
Pedunculated, highly papillary, avascular tumour covered by a layer of endothelium. Tumors resemble sea anemones when placed in normal saline.
Location
Most originate from the valves:
Aortic > Mitral > Tricuspid > Pulmonic.
Ninety-five percent in the left side of the heart [9].
Symptoms
Most patients are asymptomatic. Presentation may involve embolic events from both tumors (partial or whole) and thrombi attached to it (strokes, TIA, visual loss, angina, infarction, syncope, death), aortic or pulmonic stenosis symptoms.
Imaging
Echo: small, mobile mass which is often pedunculated. Central echolucency may be present. Tumors often appear speckled and have stippled pattern near the edges (“shimmering edge”)
CT and MRI – usually not necessary.
Lipoma (Fig. 9.4)
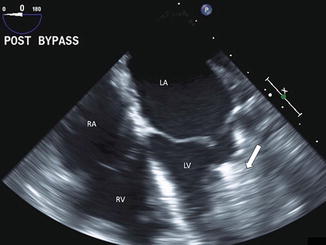
Figure 9.4
Transesophageal four chamber view showing massive cardiac lipoma (arrow) in the left ventricle which is extending into the mitral valve
Morphology
Accumulation of adipocytes
Location
50 % subendocardial origin
More frequently located in the ventricles
Symptoms
usually asymptomatic
If present, are due to arrhythmias, heart block, compression of coronary arteries
Imaging
Echo: helps with size and location
CT and MRI – may be useful for diagnosis since lipomas have distinctive fat imaging pattern
Treatment
surgery if symptomatic
N.B. Lipomatous septal hypertrophy is not a tumor, but rather a benign hyperplasia of adipose tissues in the limbus of the fossa ovalis. Since thin part of interatrial septum (fosssa ovalis) is not involved, a typical “dumbell shaped” image is seen on 2D echo
Rhabdomyoma (Fig. 9.5)
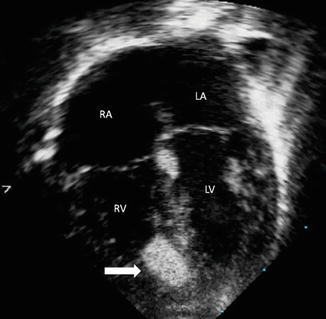
Figure 9.5
Echocardiogram (note the different orientation) showing right ventricular rhabdomyoma (arrow); orientation is inverted with atria on top and ventricles on bottom
Most common primary cardiac neoplasm in children [10].
Morphology
Microscopically consist of “spider cells” – striated cells with features of myocytes.
Tumor cells loose the ability to divide and may regress spontaneously in both size and number [1, 8, 11].
Location
Tumors are usually multiple and located in ventricles [6].
Symptoms
arrhythmias, heart block, flow obstruction
Associations
Very strong association with tuberous sclerosis, ventricular pre-excitation and Wolff-Parkinson-White syndrome [8].
Imaging
Treatment




observation (since there is often a spontaneous remission) and surgery in symptomatic patients< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
