Black-Blood Imaging
Black-blood images are produced with MR pulse sequences that null signal from flowing blood for better visualization of cardiac and mediastinal anatomy and vascular wall pathology. Techniques include conventional spin echo imaging, fast spin echo or turbo spin echo, and ultrafast single-shot turbo spin echo methods, all of which are performed with ECG gating. Preparation pulses are commonly implemented to improve image contrast. This chapter reviews implementations of conventional spin echo and faster echo train sequences, emphasizing methods for optimal blood nulling.
KEY CONCEPTS
[right half black circle] For cardiac spin echo sequences, TR is usually equal to one R-R interval for T1- or proton density-weighted images or two R-R intervals for T2-weighted images.
[right half black circle] Spin echo sequences achieve blood nulling because moving protons do not experience both the 90° excitation and 180° refocusing pulses and therefore do not contribute to the echo.
[right half black circle] When an acquisition time for a spin echo sequence exceeds a breath hold, multiple signal averages can be used to minimize respiratory motion artifacts.
[right half black circle] Fast spin echo cardiac MR images can be used for multislice imaging or for high-resolution single-slice images.
[right half black circle] Fast spin echo sequences rely on double inversion recovery pulses to null signal from flowing blood during imaging.
[right half black circle] Half-Fourier single-shot fast spin echo sequences can produce black-blood images in less than one heartbeat but require double inversion recovery pulses to null blood signal.
[right half black circle] Triple inversion recovery fast spin echo sequences generate fat-suppressed, black-blood, T2-weighted images of the cardiovascular system.
SPIN ECHO CARDIAC MR IMAGING
The principles of spin echo imaging have been presented in Chapter I-4. Recall that essential components of the spin echo pulse sequence are the 90° excitation pulse and a 180° refocusing pulse. The parameters that determine image contrast are the repetition time, TR, and the echo time, TE. For Tl-weighted imaging, the TR and TE are typically 500-800 msec and <50 msec, respectively, while for T2-weighted imaging, they are ≥1200 msec and ≥80 msec.
Spin Echo: ECG Gating
To minimize motion artifacts due to the beating heart, data for each image must be acquired during the same temporal phase of the cardiac cycle. The acquisition is synchronized to cardiac motion by using ECG gating. The TR is usually set to be equal to the R-R interval. For example, for a subject with a heart rate of 72 bpm, the R-R interval = (60 sec/min)/(72 beats/min) = 0.833 sec, and consequently, the TR would be 833 msec.
In most subjects, defining the TR as equal to one R-R interval will result in Tl-weighted imaging, provided a short TE is used. For subjects with slower heart rates, the contrast may be closer to proton density-weighted.
View Answer
Answer: By triggering off every other R wave, instead of every R wave, a longer TR can be achieved. For a subject with heart rate of 72 bpm, the TR would be 833 msec × 2 = 1666 msec. The TE also needs to be lengthened to at least 80-100 msec. Because the TR is two times the R-R interval, the T2-weighted sequence will require an acquisition time that is twice as long as that of a T1-weighted sequence.
Spin Echo: Image Contrast
For most routine black blood imaging of the heart, the TR is equal to one R-R interval. It usually does not matter whether the image contrast is strongly Tl-weighted or
closer to being proton density-weighted. The main function of these images is to provide anatomic assessment of cardiac and vascular structures in the absence of signal from flowing blood.
closer to being proton density-weighted. The main function of these images is to provide anatomic assessment of cardiac and vascular structures in the absence of signal from flowing blood.
T2-weighted sequences triggered off every other R wave may be important in certain settings such as evaluation of masses or vasculitis. To enhance conspicuity of pathology, fat suppression is often used.
IMPORTANT CONCEPT:
With ECG-gated spin echo images, the TR is usually a multiple of the R-R interval. Typically Tl-weighted or proton density-weighted images are used for anatomic imaging (TR = R-R interval), while T2-weighted images may be important for the assessment of certain types of pathology (TR = 2 R-R intervals).
Multislice ECG-Gated Spin Echo Imaging
As described in Chapter I-4, because the TE is short relative to the TR, there is ample time to collect data from multiple slice positions when performing an ECG-gated spin echo sequence (Figure III3-1).
The number of slices that can be acquired during one acquisition depends on the acquisition window and on the total number of 90°-180°-echoes that can fit into the acquisition time. The acquisition window usually corresponds to about 85% of the R-R interval (Chapter III-1).
For the subject with a heart rate of 72 bpm, the R-R interval is 833 msec, and the acquisition window is about 700 msec. If the total time from start of the 90° RF pulse to the end of the echo is 35 msec, then the number of slices that could be imaged in the same time as needed for a single slice would be 700/35 or 20 (Figure III3-1).
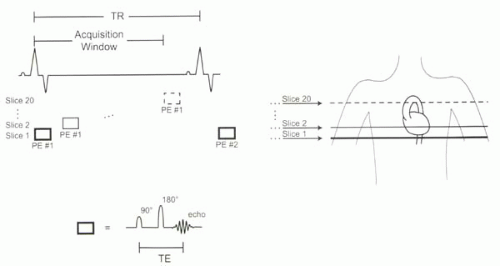 |
With an ECG-triggered spin echo sequence, the first slice position is imaged immediately after the R wave, while the last is acquired toward the end of the R-R interval. Hence, each slice will reflect the heart at a different phase of the cardiac cycle (Figure III3-1). On a series of transaxial images, the more cephalad images may be acquired during systole, and the more caudal slices may be acquired during diastole. Alternatively, the slices could be acquired in reverse order. It is important to recognize that motion artifacts are most likely to affect images collected during peak systole, while signal in the blood pool is most likely during diastole.
Acquisition Times for ECG-Gated Spin Echo Imaging
As with all spin echo imaging, acquisition times are dependent on TR. For cardiac applications, because TR
depends on heart rate or R-R interval, the total acquisition time can be expressed as:
depends on heart rate or R-R interval, the total acquisition time can be expressed as:
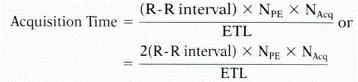
depending on whether triggering occurs with every heartbeat or every other heartbeat. With conventional spin echo imaging, a single line of k-space is acquired during each heartbeat, so that the echo train length, ETL, is equal to 1. If there are 128 phase-encoding lines, then the acquisition time for one set of data (NAcq = 1) will be 128 heartbeats. For a subject with heart rate 72 bpm, and R-R interval = TR = 833 msec, the acquisition time will be 128 × 0.833 sec = 106 sec, or nearly 2 min. If a more T2-weighted sequence is desired, then a TR equal to two R-R intervals will double the acquisition time (212 sec) to nearly 4 min.
CHALLENGE QUESTION: Acquisition times for spin echo sequences exceed the time frame for a breath hold. How can respiratory artifacts be minimized for these acquisitions?
View Answer
Answer: Averaging multiple signals, say three to four signal averages (NAcq), will minimize respiratory artifacts. Consequently, acquisition times increase proportionately by a factor of 3-4.
Spin Echo: Multiple Signals Averaged
Because acquisition times with spin echo images exceed breath holding times, subjects are usually instructed to breathe normally while multiple signals, typically three or four, are acquired and averaged. If each acquisition requires 2-4 min, then total acquisition time for multiple NAcq ranges from 6 to 16 min. For most subjects, a set of conventional spin echo images through the chest requires about 10 min.
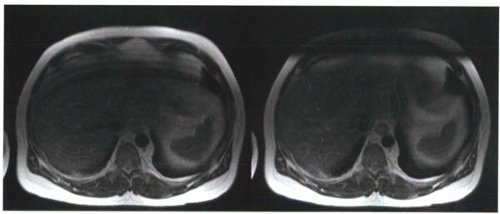 FIGURE III3-2. Spin echo images performed with multiple averages show ghosting artifacts (left) resulting from the high signal of the subcutaneous fat near the surface coils. Artifacts are reduced by placing saturation bands over the anterior abdominal wall (right). |
Despite the use of signal averaging, respiratory motion still frequently causes artifacts on conventional spin echo images. Most commonly, these artifacts arise from ghosting from the subcutaneous fat of the anterior chest or abdominal wall (Figure III3-2). Saturation bands placed over the ghosting source are used to reduce these artifacts (Chapter I-9).
Spin Echo Black-Blood Effects
To generate a spin echo, protons must experience both the 90° excitation pulse and the 180° refocusing pulse. If the RF pulses are slice selective and if the protons in the blood are not present within the slice long enough to experience both RF pulses, then no echo is generated, resulting in a signal void. For this reason, flowing blood is typically black with conventional spin echo imaging. As discussed in Chapter II-1, to minimize the signal from flowing blood, several strategies can be employed: using a longer TE, thinner slices, and slice positioning orthogonal to the direction of flow. Moreover, acquisitions during systole, when flow is fastest, have more complete nulling of flowing blood.
CHALLENGE QUESTION: Consider routine axial images of the heart using spin echo imaging. How does the order of acquisitions (cranial to caudal or caudal to cranial) affect the image quality and degree of blood nulling on the images?
View Answer
Answer: The images acquired immediately after the R wave will be in systole and have best blood nulling on spin echo




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
