Fig. 6.1
Diagram of the patient’s auscultation findings including a prominent ejection click, a diastolic crescendo decrescendo murmur and systolic decrescendo murmur
Test Results
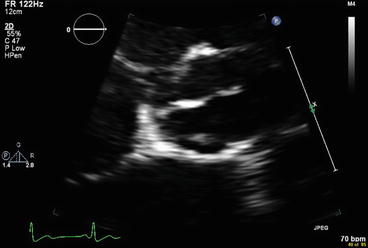
Echocardiogram:
Normal left ventricular size and function.
The aortic root diameter is upper normal (3.6 cm).
Echo Doppler shows mild AR and mild AS (2.1 m/s).
Clinical Basics
Definition
Most commonly, a BAV is associated with the congenital fusion of right and left coronary cusps, which is seen in 70–80 % of cases (Fig. 6.4). The other, less common fusion is of the right cusp and the posterior (noncoronary) cusp, which is seen in the other 20–30 % of cases [1].
Fig. 6.4
There are several types of malformations characteristic of a bicuspid aortic valve
Median raphe is typically (60 %) in the conjoint cusp. Differential point for acquired bicuspid AV: Raphe does not reach cusp margin.
Prevalence
BAV is a congenital disorder that affects 1–2 % of the population [2]. Males make up 70–80 % of cases. It is the most prevalent congenital heart abnormality.
Etiology
BAV accounts for approximately half of all cases of AS, with a presentation typically in the 5th–6th decade. It also accounts for about one-fourth of all cases of AR, commonly presenting earlier in life.
A 2012 study of patients at necropsy found that 61 % of those with BAV had aortic stenosis [3, 4]. There is a significant association with aortic dilatation, with studies varying from 33 to 79 % prevalence depending on the study criteria. Increased risk for endocarditis has also been associated with BAV [4].
There does appear to be a significant genetic component to BAV. One epidemiological study showed a prevalence of 14.6 % of BAV in affected families, which is a much higher rate than the general population [5]. The risk of BAV among 1st degree relatives of an affected individual is 10 % [2]. A family history of BAV should raise suspicions during evaluation.
There is also a high association of BAV with other congenital anomalies including aortic coarctation, interrupted aortic arch, and other aortopathies [2].
Signs and Symptoms
Commonly asymptomatic and may be found as an incidental finding on an echo for another reason.
Symptoms of BAV are related to the pathologies closely associated with the anomaly, including AR, AS, and aortopathies.
Key Auscultation Features
There are several key auscultation features associated with BAV [6]. Table 6.1 describes the auscultation characteristics of the anomaly.
Table 6.1
Key auscultation characteristics associated with BAV
Feature
Description
S1 is split in 85 % of cases
Ejection click in BAV associated with aortic valve opening
Halting of opening of AV
Intensity equal to or greater than M1
Intensity constant throughout respiration
Heard over entire precordium
At apex, true “splitting” of S1 is generally not audible
Associated with a loud A2
Short and sharp ejection “click”
Timing:
T1 <50 ms (pa-da)
A1 >50 ms (pa-ta)
Mitral/tricuspid closure represents non-pathological splitting
Systolic murmur
Early to mid systolic
Flow related
S2
Increased 1.5–2 fold in uncomplicated BAV
A decrease might suggest a degree of AS
Diastolic murmur
AR is common
Frequently mild
It is important to differentiate between non-pathological splitting of S1 and a true ejection click. A true BAV ejection click is related to the halting of the opening of the aortic valve, and the sound occurs later than a typical split S1 (Fig. 6.5).
Fig. 6.5
Phonogram of aortic ejection click heard in bicuspid aortic valve. Note the timing of the click relative to M1 and T1, distinguishing it from non-pathological splitting of S1. Note also the loud S2 (Used with permission from Leech et al. [6])
One should also note that the auscultatory hallmarks of BAV may vary depending on whether aortic stenosis or regurgitation is present.
Auscultation examples of bicuspid aortic valve.
Click here to listen to an example of bicuspid aortic valve showing an ejection click, with a mild (15 mmHg) gradient, and see an image of the phonocardiogram (Video 6.1).< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


