Described are findings in a 70-year-old man who had heart transplantation 4 years after treatment with a left ventricular assist device, and surgical closure of his previously replaced aortic valve. The result was a totally nonfunctioning left ventricle resulting in severe atrophy.
Exercise enlarges our noncardiac striated muscles and disuse atrophies them. The same would appear to be the case with cardiac muscle. We recently studied a very small heart of a very large man who 4 years earlier had undergone insertion of a left ventricular assist device (LVAD) with surgical closure of his previously replaced aortic valve. This report describes findings in this patient in whom the LVAD totally replaced his left ventricular (LV) function.
Description of Patient
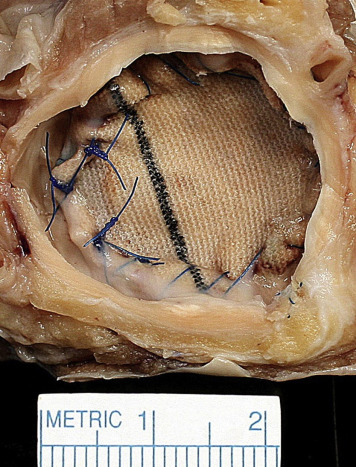
This 70-year-old man, who was born in June 1945, underwent heart transplantation (HT) because of severe heart failure in July 2015. His symptoms of heart failure began when he was aged 45 years. At age 55 years, he underwent aortic valve replacement with a St. Jude Medical prosthesis for aortic stenosis involving a congenitally bicuspid aortic valve. Because of worsening heart failure when he was aged 65 years (2011), an HeartMate 2 LVAD was inserted, and an occluding patch was placed on the aortic aspect of the prosthesis in the aortic valve position preventing blood flow into the aorta through the prosthetic valve ( Figure 1 ). These endeavors resulted in some improvement in symptoms. Because of chronic atrial fibrillation, he underwent an ablation procedure on 3 occasions. Because of severe heart failure, HT was performed at age 70 years. By 2 months postoperatively, he had resumed near-normal activities. He was 78-inch tall, and his maximum weight was 250 pounds (body mass index 28 kg/m 2 ).
The operatively excised native heart weighed 280 g and contained several scars in the posterolateral LV wall despite a wide-open dominant right coronary artery ( Figure 2 ). In contrast, the left anterior descending and left circumflex coronary arteries were severely narrowed by plaque. Histologic study of sections of the LV wall showed thinning of numerous myofibers ( Figure 3 ).


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


