Fig. 43.2 The amplitude of the fibrillatory waves in atrial fibrillation (AF). As a generalization, at the onset of AF, the f waves are of large amplitude (red); after days–weeks, the amplitude declines (blue), becoming quite small after weeks–months (orange). In long standing AF the baseline is often quite flat (green) – the clue to the presence of AF is not so much the f waves, as the regularity or otherwise of the QRS complexes. In AF the QRS complexes occur irregularly, as there is no pattern to the electrical bombardment of the atrioventricular (AV) node, whereas in sinus rhythm and arrhythmias other than AF the RR interval is usually fairly constant.
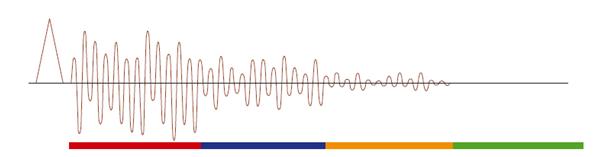
Fig. 43.3 At the onset of atrial fibrillation the heart rate is high, and can sometimes, as in this example, be surprisingly regular (giving rise to symptoms of regular rather than irregular palpitations). However, careful inspection (for example, by mapping out the RR intervals on a piece of paper) shows that the RR intervals vary continuously – a key clue as the fibrillatory ‘f’ waves are so fine as to hardly be visible.

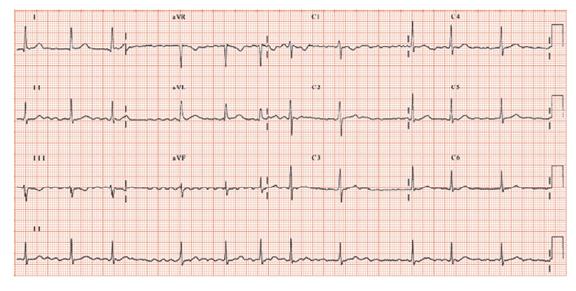
Fig. 43.4 Atrial fibrillation (AF). The clue that the rhythm is AF is not the fibrillatory waves – they are rather small – but the irregularly irregular heart rate. The heart rate is very well controlled, due to: (i) possibly intrinsic disease of the atrioventricular (AV) node; (ii) drugs, such as a beta-blocker (digoxin is unlikely here as there are no ST/T waves changes); (iii) AF being long standing. The QRST complexes are normal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


