Anatomy in Clinical Electrophysiology
An understanding of cardiac anatomy is essential to the diagnosis and treatment of arrhythmias. This knowledge is required to allow recording of normal and abnormal electrical activity as well as anticipate electrophysiological consequences of various types of cardiac pathology.
Right Atrium
Normal electrical activation of the heart begins in the sinus node complex located as a subepicardial structure at the junction of the high right atrium (RA) and the superior vena cava (see Fig. 1-1). The sinus node is a spindle-shaped complex of cells that generally lies in a superior and lateral location in the RA but occasionally extends posteromedially to the interatrial groove. The right phrenic nerve runs in close proximity to the sinus node on the epicardial surface of the RA. The sinus node is supplied by the right coronary artery (RCA) in 60% of patients and left circumflex artery (LCX) in 40% of patients (see Table 1-1). The sinus node is heavily innervated by parasympathetic and sympathetic inputs.
Once the impulse leaves the sinus node it travels inferiorly toward the atrioventricular (AV) node located in the low septal aspect of the RA. Conduction to the left atrium occurs through activation of the coronary sinus (CS) and through a series of fibers called the Bachmann bundle that extend from the crest
of the right atrial appendage through the transverse sinus behind the aorta and across the interatrial groove toward the left atrial appendage (LAA) (see Fig. 1-2). There is also some activation through the fossa ovalis.
of the right atrial appendage through the transverse sinus behind the aorta and across the interatrial groove toward the left atrial appendage (LAA) (see Fig. 1-2). There is also some activation through the fossa ovalis.
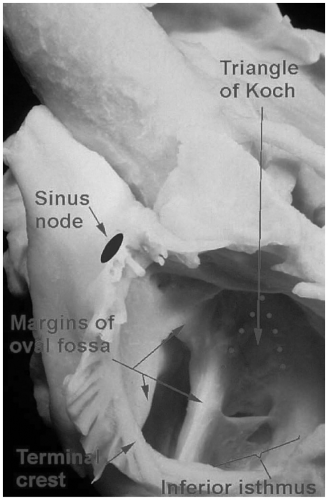 FIGURE 1-1. Right atrium opened, demonstrating the epicardial location of the sinus node in relation to the crista terminalis (terminal crest). The fossa ovalis and triangle of Koch are also demonstrated. (Courtesy Prof RH Anderson) (See color insert.) |
TABLE 1-1 Vascular Supply of the Cardiac Conduction System
| RCA, right coronary artery; LCX, left circumflex artery, AV, atrioventricular node; LAD, left anterior descending coronary artery. |
|
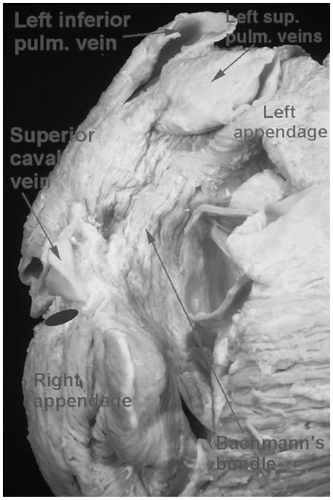 FIGURE 1-2. Right atrium demonstrating the location of the Bachmann bundle. The blue oval represents the sinus node. (Courtesy Prof RH Anderson) (See color insert.) |
The ostium of the CS lies in an inferior and posterior location in the RA. It forms the base of the triangle of Koch within which lies the compact AV node. The two sides of this triangle which emanate from this base include the septal leaflet of the tricuspid valve (TV) and the tendon of Todoro. The tendon of Todoro is a fibrous structure that forms as an extension of the Eustachian valve of the inferior vena cava and the Thebesian valve of the CS ostium (see Fig. 1-3). This tendon runs septally into the central fibrous body (CFB). The CFB is a confluence of fibrous tissue formed by the connection of the membranous septum with the fibrous trigones. The right and left fibrous trigones represent the areas of thickening at the edges of the connected or shared aspects of the aortic and mitral valves (anterior mitral leaflet). The right fibrous trigone connects with the membranous septum to form the CFB. The right coronary cusp of the aortic valve overlies and is continuous with the membranous septum. The noncoronary cusp overlies the right fibrous trigone and the left
coronary cusp overlies the left fibrous trigone. The aortic-mitral curtain is suspended between the trigones and forms the posterior aspect of the aortic outflow tract (see Fig. 1-4).
coronary cusp overlies the left fibrous trigone. The aortic-mitral curtain is suspended between the trigones and forms the posterior aspect of the aortic outflow tract (see Fig. 1-4).
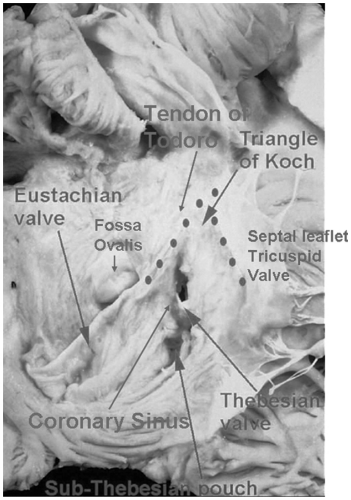 FIGURE 1-3. Demonstration of the boundaries of the triangle of Koch, right atrium, and fossa ovalis. (See color insert.) |
The fossa ovalis is the rim demarcating closure of the septum secundum and remnant of the septum primum. It is roughly at a 90-degree angle from but at the same level as the AV node/His bundle. The roof of the fossa ovale is formed by a muscular ridge called the limbus. Direct placement of a needle through the fossa will lead to the left atrium (Fig. 1-3). Penetration anterior to the fossa will enter the aorta. Penetration posterior and superior to the fossa will enter the invaginated groove or cleft between the right and left atria. This is the space commonly used by surgeons to access the left atrium and mitral valve.
The crista terminalis is a thick fibrous band of tissue that connects the inferior and superior vena cavae. It is located in the posterolateral aspect of the RA and can be identified by characteristic fractionated or split electrical recordings during electrophysiology study. This structure is a particularly common site for the development of atrial tachycardia.
The right atrial appendage is a relatively large structure which lies on the anterolateral surface of the left atrium. As is true of most of the RA it is full
of pectinate muscles. The shape of this structure facilitates stable pacemaker lead placement; however, its proximity to the TV sometimes results in “far field” sensing of ventricular electrical activity.
of pectinate muscles. The shape of this structure facilitates stable pacemaker lead placement; however, its proximity to the TV sometimes results in “far field” sensing of ventricular electrical activity.
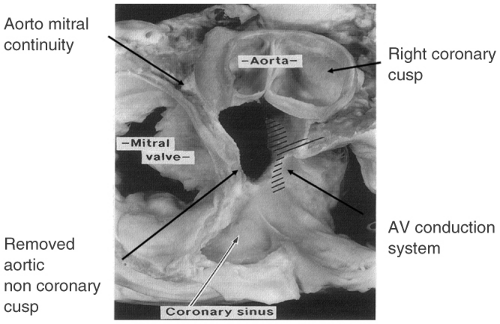 FIGURE 1-4. Cross-section of the heart with the noncoronary cusp of the aortic valve removed. The relationship of the mitral valve, aortomitral continuity, aortic valve, and atrioventricular (AV) conduction system is shown.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|