Chapter 69 Ambulatory Electrocardiography
Long-Term Monitors and Event Recorders
Types of Ambulatory Electrocardiography Monitors
Continuous Short-Term Monitors
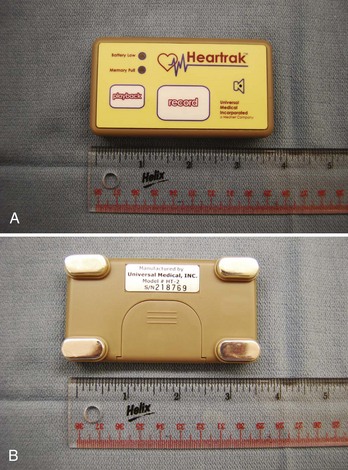
The Holter monitor, invented by Neil Holter in 1941, is the prototype for continuous ambulatory ECG monitors. Modern continuous monitors provide three to 12 high-quality surface ECGs with full disclosure for a period of 24 to 48 hours. These are battery-operated, self-contained devices that comprise electrodes and leads connected to a compact, lightweight box that can be worn on the patient’s belt or placed in a pouch. These devices are capable of storing high-quality ECG data on a cassette tape, which can then be turned in and analyzed at a workstation. More recently, continuous monitors store high-fidelity digital ECGs on a flash card or a PC card. Time stamps correlating patient symptoms to the ECG, extended battery and memory capacity (up to 96 hours), ability to transmit digital recordings over the Internet, and software packages facilitating “advanced” digital ECG analyses are also available. This type of monitor is ideal for patients who have symptoms that occur frequently (at least once per day) but has limited application in situations where patients experience rare and sporadic symptoms. An example of a Holter monitor is shown in Figure 69-1.

Event Monitors
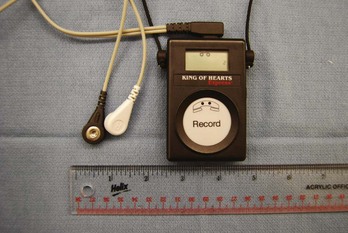
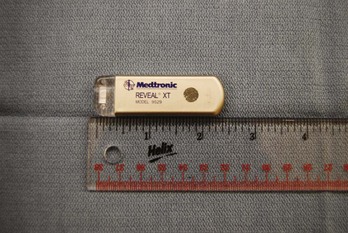
Event monitors are ambulatory ECG monitors that are designed to be worn or carried for up to 30 days. Two types of event monitors are available: (1) Loop recorders (before symptom onset) constantly store and dump ECG data for 30 seconds to 4.5 minutes (depending on the manufacturer); when activated by the patient, ECG data from this buffer are stored for analysis, along with an interval of ECG that is recorded after activation. This type of monitor requires that the patient wear electrodes and leads constantly. (2) Nonlooping event recorders (after symptom onset) do not require that the patient wear electrodes continuously. These are small recording devices that are kept by the patient nearby (pocket or purse), and when the patient has symptoms, the electrodes on the device are placed on the chest, and the ECG is then recorded. These devices typically have 5 to 10 minutes of memory, but more advanced devices may have up to 30 minutes of memory capacity. Event recorders are ideal monitors for identifying a symptom/rhythm correlation for intermittent symptoms that are long enough to allow time for recording. The limitations of event recorders are that patient-triggered recorders cannot detect asymptomatic arrhythmias. Looping event recorders with automatic triggers may allow the detection of very slow or very rapid arrhythmias but may “miss” some arrhythmias such as rate-controlled atrial fibrillation (AF) or supraventricular tachycardia (SVT) that are slower than the detection rate of the device. The primary limitations of looping event recorders are patient discomfort, poor patient compliance, and premature termination of monitoring (since patients often complain about having to wear electrodes and leads for extended periods). The limitations of nonlooping event recorders include their inability to detect short-lived arrhythmias or event initiation and occasional poor ECG quality. Examples of a looping event recorder and a nonlooping event recorder are shown in Figures 69-2 and 69-3, respectively.
Implantable Loop Recorders
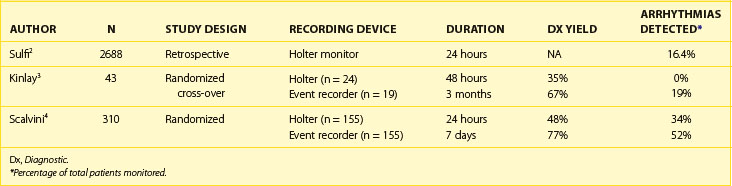
Implantable loop recorders (ILRs) are small, lightweight devices that are placed in the subcutaneous space in a minor procedure and provide high-quality ECGs. The earlier-generation ILRs were equipped with patient-activated storage only (Medtronic Reveal; Medtronic, Inc., Minneapolis, MN). Subsequent models have implemented programmable auto-triggering based on high and low heart rate thresholds (Reveal Plus [Medtronic]; Confirm [St Jude Medical, St. Paul, MN]; Sleuth [Transoma Medical, Arden Hills, MN]). The most-recent-generation ILRs are equipped with AF detection algorithms (Reveal XT, AF [Medtronic]). These devices provide 1 to 3 years of monitoring with 48 to 630 minutes of storage and can be patient activated or automatically activated by programming a low rate and a high rate for detection. In the case of patient-activated recordings, these devices store 60 to 240 seconds of ECGs before (usually 60 seconds of ECGs) and after the patient has triggered the device. The ECGs corresponding to these events can be reviewed noninvasively. Some devices are equipped with remote recording capabilities, by which ECGs from the recorder can be sent transtelephonically to a receiving station (Confirm) or can be manually or automatically transmitted from a home-based station to a secure Web site (Reveal Plus and Carelink [Medtronic]) or to a monitoring station manned by trained ECG technicians (Sleuth). These devices are ideal for rare, but significant, events that are worrisome in the case of a cardiac arrhythmia such as syncope. The limitations of these monitors include failure of the patient to activate the device during symptoms, availability of only one lead for analysis, discomfort associated with the implantation and removal of the device, a small risk of infection, and minor cosmetic alteration of the chest wall. An example of an ILR is shown in Figure 69-4.
Implantable Pacemakers and Implantable Defibrillators
Implantable defibrillators and pacemakers are placed for therapeutic, rather than diagnostic, reasons, but they do have sophisticated diagnostic capabilities that allow for storage of intracardiac ECGs during tachyarrhythmias. Diagnostic information available from implantable devices includes rate histograms, atrial high-rate episodes, ventricular high-rate episodes, and stored intracardiac ECGs (depending on the model and vendor of the device). The accuracy of the information available in the device depends on appropriate sensing parameters and programmed detection parameters. Diagnostic information about arrhythmic events that are available in cardiac pacemakers and implantable defibrillators is discussed in Chapters 22 and 92 and therefore will not be covered in this chapter.
Diagnostic Efficacy of Ambulatory Electrocardiography Monitors
Palpitations
Palpitations, defined here as an awareness of one’s heart beat, are a symptom commonly encountered in clinical practice. Although possibly a manifestation of arrhythmias, palpitations are often caused by noncardiac factors. When arrhythmias are the cause of palpitations, the most common rhythms recorded during symptoms are premature atrial contractions, premature ventricular contractions, SVTs, and AF. In a prospective cohort study, 190 patients who presented at an academic medical center with palpitations were evaluated and followed up for 1 year. A diagnosis of the etiology of their palpitations was established in 84%. Among these patients, 40% experienced palpitations because of cardiac arrhythmias and 33% because of anxiety and panic disorder, and the remaining patients had nonarrhythmic causes.1 Patients with palpitations associated with structural heart disease (including complex congenital heart disease), presyncope, or syncope are at higher risk of having a cardiac arrhythmia, which may even be life threatening.
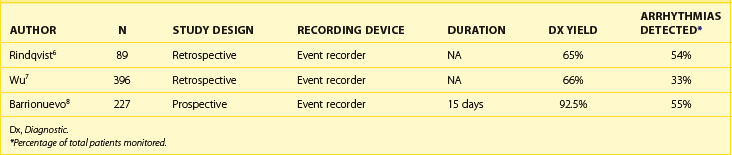
A limitation of some studies evaluating the diagnostic efficacy of continuous 24- to 48-hour monitors for the workup of palpitations is that some of these studies report the number of times these monitors provide an arrhythmia diagnosis but not the number of times the palpitations are associated with sinus rhythm. This underestimates the diagnostic yield of the 24-hour Holter monitor because multiple recordings of sinus rhythm associated with palpitations may help rule out cardiac arrhythmia as the cause of the palpitations (Tables 69-1, 69-2, and 69-3).

Diagnostic Yield of 24-Hour Continuous Electrocardiography Monitors
In general, the likelihood of a 24-hour Holter monitor documenting arrhythmias in patients with intermittent palpitations is low. In a large retrospective study of consecutive patients who received Holter monitors for symptoms of palpitations, the 24-hour Holter monitor demonstrated sinus rhythm in 2247 of 2688 Holter recordings (83.6%). Two hundred seventy-six patients had a second Holter monitoring performed, and 210 of 276 were negative (76.1%). Among patients with arrhythmias corresponding to palpitations detected on 24-hour Holter monitoring, 4.4% had frequent ectopic beats (>15 per 10,000 beats), 6.6% had AF, 2.8% had narrow-complex tachycardia, and 2.6% had ventricular tachycardia (VT). The frequency of cardiac arrhythmias detected by 24-hour Holter monitoring is especially low among patients younger than 50 years, in whom 93.1% of Holter monitors demonstrated no arrhythmias. Cardiac arrhythmias were observed in 29% of patients older than 70 years, with 15% of recordings demonstrating AF.2 This study provided information about the type of arrhythmias recorded during continuous 24-hour monitoring among patients with palpitations. The study did not provide insights into the diagnostic yield of the Holter monitor (the ability to provide a symptom/rhythm correlation).
Diagnostic Yield of Continuous Monitors and Event Recorders
In a randomized cross-over study of 43 patients with intermittent palpitations, patients were randomized to a 48-hour Holter monitor versus a 3-month (nonlooping) event recorder and then crossed over to the other monitor. The 48-hour Holter monitor recorded ECGs during symptoms in 15 (35%) of 43, and none of these recordings demonstrated an arrhythmia. The event recorder was able to record ECGs during symptoms in 29 (67%) of 43 and diagnosed an arrhythmia in 8 (28%) of 29. Among the arrhythmias recorded on the event recorder, SVT, premature ventricular beats, and AF or atrial flutter accounted for 18%, 12%, and 6% of arrhythmias, respectively.3 Scalvini et al randomized 310 patients with palpitations to initial monitoring with a 24-hour Holter monitor (n = 155) or a looping event recorder for 7 days (n = 155). The diagnostic yield of the Holter monitor was 48% (34% of patients had arrhythmias detected) and 77% for the event recorder (52% of patients had arrhythmias detected, P < .01).4 In a review of studies evaluating the diagnostic yield of ambulatory ECG monitors for palpitations, Zimetbaum et al reported a diagnostic yield (providing a symptom/rhythm correlation) of 66% to 83% for event recorders and 33% to 35% for a Holter monitor.5
In noncomparison studies, nonlooping event recorders have demonstrated a diagnostic yield for palpitations of up to 66% with arrhythmias detected in 33% to 54% of patients.6–8 Studies of looping event recorders have demonstrated a diagnostic yield of 66% to 83% with arrhythmias detected in 28% to 42% of patients.9,10
Olsen et al evaluated the role of mobile cardiac outpatient telemetry (MCOT, Cardionet, Philadelphia, PA) in the evaluation of palpitations, syncope, and presyncope. In 18 patients in this study, MCOT was the first monitoring system applied for the evaluation of palpitations. The diagnostic yield was 73% (14 of 18) with all 14 patients recording arrhythmias. In another 58 patients, a previous rhythm diagnosis associated with palpitations was already established with another recording system prior to MCOT monitoring. During monitoring, 34 (59%) of 58 of patients had a symptom/rhythm correlation, with 27 (79%) of 34 demonstrating an arrhythmia associated with palpitations.11 These data demonstrate the limitations in evaluating patients for palpitations. Only 59% of patients with a previously established “diagnosis” of an arrhythmia had recurrent palpitations during a long-term monitoring period, and an arrhythmia different from the original “diagnosis” was responsible for palpitations in many patients. These observations should be considered when making clinical decisions about arrhythmias detected by any ambulatory monitor and in the interpretation of studies evaluating the diagnostic yield of these monitors for palpitations.
Optimal Duration of Monitoring for Palpitations
Data on the optimal duration of monitoring in providing a symptom/rhythm correlation demonstrate that 2 weeks of monitoring yields the majority of diagnoses. In a study by Reiffel et al, the weekly yield of an event recorder was evaluated retrospectively in 5052 patients. During the first 2 weeks of monitoring, 87% of patients had transmitted an ECG recording during symptoms. The additional diagnostic yield during the following 2 weeks (weeks 2 to 4) was 9%.12 Zimetbaum et al demonstrated that 83% of patients had a diagnostic transmission from their event recorder within 2 weeks of monitoring and that the diagnostic yield was low beyond this monitoring period.13 On the basis of this evidence, a monitoring period of at least 2 weeks and up to 4 weeks is considered to provide a symptom/rhythm correlation in the majority of cases of diagnosis likely to be achieved by an event recorder.
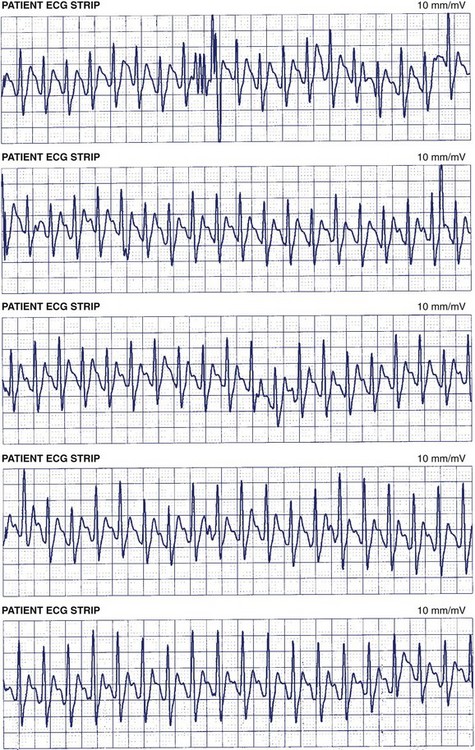
To summarize this section, studies of the etiology of palpitations demonstrate that nonarrhythmic causes of palpitations are common. ECG recordings during palpitations may demonstrate different arrhythmias during different episodes of palpitations within the same patient. With these data in mind, event recorders with patient-triggered events provide better diagnostic yield than does a 24- to 48-hour Holter monitor and will provide a diagnosis in up to 87% of patients within the first 2 weeks of monitoring (Figure 69-5). The continuous 24-hour monitor is associated with a relatively low diagnostic yield (approximately 35%) among patients with intermittent palpitations, and the second 24-hour recording is of especially low yield. ILRs and mobile cardiac telemetry are not indicated in most cases of intermittent palpitations, as they are not likely to provide additional diagnostic yield to external event recorders.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


