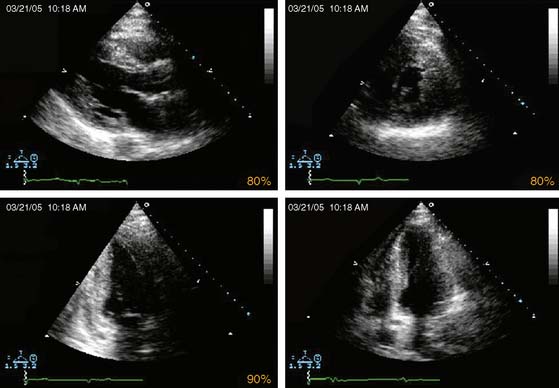
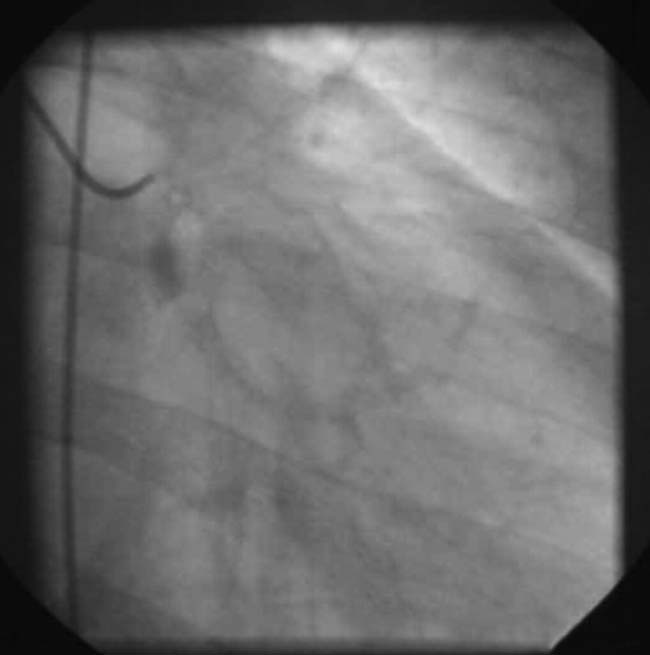
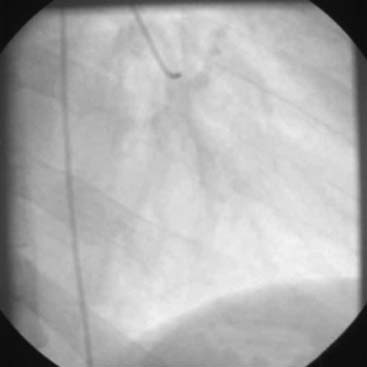
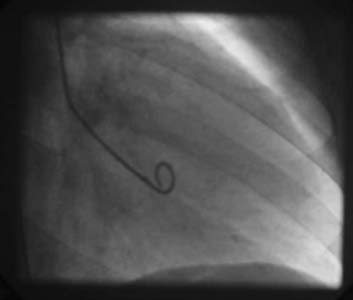
Case 35 A 53-year-old African American male was admitted to the hospital with complaints of shortness of breath and dizziness. He was diagnosed with hypertension 4 to 5 years earlier and is receiving treatment. He also has hyperlipidemia and remote history of smoking. He has history of palpitations since childhood. There is family history of sudden death. His one brother died suddenly at age 43 years. ECG showed normal sinus rhythm with marked left ventricular hypertrophy, generalized ST-segment depression, and deep T-wave inversions in precordial as well as limb leads. His ECG is shown next. What is your interpretation? (Video 1) Echo shows severe left ventricular hypertrophy (LVH). Left ventricular ejection fraction (LVEF) is 65% to 70%, without evidence of regional wall-motion abnormalities. He was ruled out for acute myocardial infarction, but because of a very abnormal echocardiogram, he underwent cardiac catheterization and coronary angiography. This is shown next. (Video 2) (Video 3) (Video 4) Coronary arteries are normal with no luminal obstruction. LV cavity is small, and the LV is hyperdynamic, with cavity obliteration in the distal part of the LV during systole. He was referred for exercise perfusion imaging to detect any exercise-induced arrhythmias and exercise-induced perfusion abnormalities. He was receiving verapamil. Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Cardiac Neurotransmission Imaging: Single-Photon Emission Computed Tomography 6 Myocardial Perfusion Imaging with Contrast Echocardiography Digital/Fast SPECT: Systems and Software Stay updated, free articles. Join our Telegram channel Join Tags: Clinical Nuclear Cardiology State of the Art and Future Direction Jun 11, 2016 | Posted by admin in CARDIOLOGY | Comments Off on 35 Full access? Get Clinical Tree
Case 35 A 53-year-old African American male was admitted to the hospital with complaints of shortness of breath and dizziness. He was diagnosed with hypertension 4 to 5 years earlier and is receiving treatment. He also has hyperlipidemia and remote history of smoking. He has history of palpitations since childhood. There is family history of sudden death. His one brother died suddenly at age 43 years. ECG showed normal sinus rhythm with marked left ventricular hypertrophy, generalized ST-segment depression, and deep T-wave inversions in precordial as well as limb leads. His ECG is shown next. What is your interpretation? (Video 1) Echo shows severe left ventricular hypertrophy (LVH). Left ventricular ejection fraction (LVEF) is 65% to 70%, without evidence of regional wall-motion abnormalities. He was ruled out for acute myocardial infarction, but because of a very abnormal echocardiogram, he underwent cardiac catheterization and coronary angiography. This is shown next. (Video 2) (Video 3) (Video 4) Coronary arteries are normal with no luminal obstruction. LV cavity is small, and the LV is hyperdynamic, with cavity obliteration in the distal part of the LV during systole. He was referred for exercise perfusion imaging to detect any exercise-induced arrhythmias and exercise-induced perfusion abnormalities. He was receiving verapamil. Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Cardiac Neurotransmission Imaging: Single-Photon Emission Computed Tomography 6 Myocardial Perfusion Imaging with Contrast Echocardiography Digital/Fast SPECT: Systems and Software Stay updated, free articles. Join our Telegram channel Join