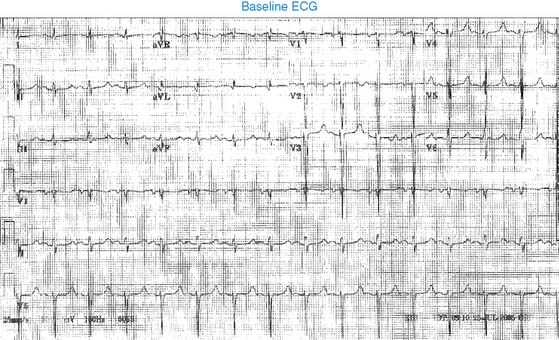
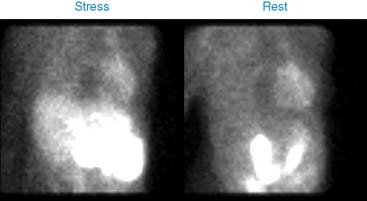
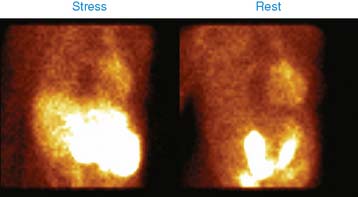
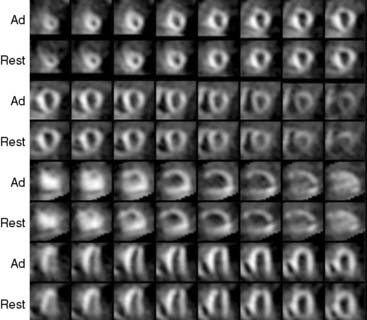
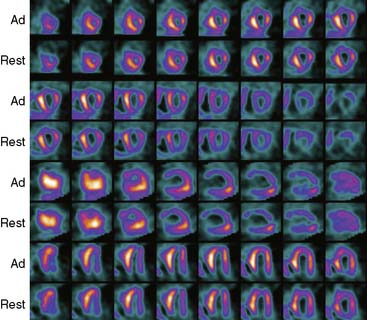
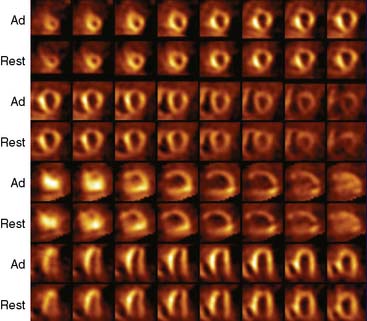
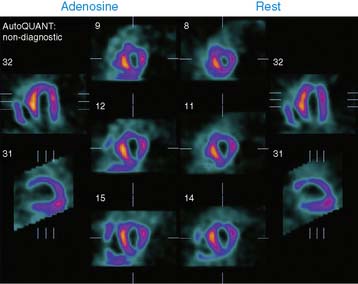
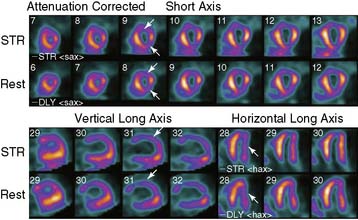
Case 20 A 43-year-old woman is admitted to the hospital for evaluation of chest pain. She had a prior history of hypertension, peripheral vascular disease, coronary artery disease, congestive heart failure, and defibrillator implant for primary prevention. She underwent coronary artery bypass grafting and pericardial stripping 12 years earlier. The details of this surgery and the indication are not available. Six years earlier, she underwent multivessel angioplasty in another hospital. She also had end-stage renal disease and was on hemodialysis. During her current admission to the hospital with chest pain, acute myocardial infarction was ruled out, and she was sent for pharmacologic stress perfusion imaging. She was on diltiazem, carvedilol, and pantoprazole. She underwent 2-day rest/stress perfusion imaging using 25 mCi of 99mTc-sestamibi on both days. Pharmacologic stress was carried out using 5-minute adenosine infusion protocol. Her heart rate remained unchanged at 86 beats/min, and blood pressure changed from 144/64 to 122/63 mm Hg. There was no chest pain with adenosine infusion. (Fig. 1) Her baseline electrocardiogram showed normal sinus rhythm. There was poor R-wave progression from V1 to V3, suspicious of an old anteroseptal myocardial infarction, and there were Q-waves in leads I and aVL, indicative of old lateral wall infarction. Electrocardiogram did not show changes from baseline with adenosine infusion. (Video 1a) (Video 1b) (Fig. 2a) (Fig. 2b) (Fig. 2c) (Video 2) (Fig. 3) Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Cardiac Neurotransmission Imaging: Single-Photon Emission Computed Tomography 6 Myocardial Perfusion Imaging with Contrast Echocardiography Digital/Fast SPECT: Systems and Software Stay updated, free articles. Join our Telegram channel Join Tags: Clinical Nuclear Cardiology State of the Art and Future Direction Jun 11, 2016 | Posted by admin in CARDIOLOGY | Comments Off on 20 Full access? Get Clinical Tree
Case 20 A 43-year-old woman is admitted to the hospital for evaluation of chest pain. She had a prior history of hypertension, peripheral vascular disease, coronary artery disease, congestive heart failure, and defibrillator implant for primary prevention. She underwent coronary artery bypass grafting and pericardial stripping 12 years earlier. The details of this surgery and the indication are not available. Six years earlier, she underwent multivessel angioplasty in another hospital. She also had end-stage renal disease and was on hemodialysis. During her current admission to the hospital with chest pain, acute myocardial infarction was ruled out, and she was sent for pharmacologic stress perfusion imaging. She was on diltiazem, carvedilol, and pantoprazole. She underwent 2-day rest/stress perfusion imaging using 25 mCi of 99mTc-sestamibi on both days. Pharmacologic stress was carried out using 5-minute adenosine infusion protocol. Her heart rate remained unchanged at 86 beats/min, and blood pressure changed from 144/64 to 122/63 mm Hg. There was no chest pain with adenosine infusion. (Fig. 1) Her baseline electrocardiogram showed normal sinus rhythm. There was poor R-wave progression from V1 to V3, suspicious of an old anteroseptal myocardial infarction, and there were Q-waves in leads I and aVL, indicative of old lateral wall infarction. Electrocardiogram did not show changes from baseline with adenosine infusion. (Video 1a) (Video 1b) (Fig. 2a) (Fig. 2b) (Fig. 2c) (Video 2) (Fig. 3) Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related Related posts: Cardiac Neurotransmission Imaging: Single-Photon Emission Computed Tomography 6 Myocardial Perfusion Imaging with Contrast Echocardiography Digital/Fast SPECT: Systems and Software Stay updated, free articles. Join our Telegram channel Join