Fig. 3.1
The normal mechanics of respiration. As the (intact) chest wall expands outward under the influence of the respiratory muscles (including the intercostal muscles), the diaphragm contracts and lowers, creating a negative intrathoracic pressure, and in response air enters through the upper respiratory system. In expiration, the process is reversed
Anatomically, a flail segment is a part of the chest wall which has lost its continuity with the chest wall and usually results from multiple rib fractures. In simple terms, it can be defined as a fracture of three or more ribs at two or more places. The literature also supports the definition of flail chest as a fracture of two or more ribs at two or more places (Fig. 3.2). The common factor in both definitions is the presence of an unstable segment, which is not continuous with the chest wall and moves in a paradoxical fashion—inward during inspiration and outward during expiration. Splinting of muscles early in the course may conceal the rib motion, and hence, this paradoxical motion could be missed. Also, induction of mechanical ventilation may also conceal the flail segment as paradoxical motion is minimized. Paradoxical movement of the flail segment occurs mainly because of two factors: loss of anatomical continuity and the effect of the negative intrapleural pressure acting on the detached segment (Fig. 3.3). Similarly flail segments of the sternum and vertebrae have also been reported, with the underlying mechanism largely remaining the same.
Fig. 3.2
Illustration of a flail chest injury—three or greater adjacent ribs with segmental fractures is a generally accepted definition (see also Chap. 1)
Fig. 3.3
Paradoxical breathing occurs when instability (i.e., from multiple rib fractures) causes inward motion of the chest wall in response to the generation of negative intrathoracic pressure (see Fig. 3.1). Expiration causes a similarly dysfunctional expansion of the unstable chest wall
The flail segment occurs after compressive forces are applied to the chest, with the thorax able to withstand about 20 % volume compression before a rib fracture can occur. In one of the studies conducted on cadavers, ribs were fractured by opening a median sternotomy with a retractor. The authors proposed that the ribs in the posterior region along with their vertebral articulations function like a lever and act as a single unit. Any force over the anterior chest wall hence results in the fracture of the ribs not only over the weaker lateral aspect but also over the posterior region near the costotransverse process articulation [11]. Anatomically, the presence of right-sided rib fractures (the eighth and below) is associated with a probability of 19–56 % of underlying liver injury, and the presence of left-sided rib fractures is associated with a 22–28 % probability of splenic injury [10]. Involvement of respiratory muscles is also a very important contributory factor in the pathophysiology of the flail chest. Hence, it is apt at this juncture to briefly discuss the muscles involved in respiration.
Inspiratory Muscles
The diaphragm is the most important inspiratory muscle; it is dome shaped having a central cartilaginous and peripheral muscular portion and forms a thin but effective boundary between the thoracic and abdominal cavity. It is inserted on the lower ribs and receives its sensory nerve supply by the phrenic nerve (C3–C5) over the central region, whereas the peripheral portion of the diaphragm is supplied by the lower 6–7 intercostal nerves. Contraction of the diaphragm increases the dimensions of the chest wall in almost all directions and forces the abdominal contents forward and downward. The diaphragm may move anywhere between 1 and 10 cm depending upon the depth of respiration. Upward movement of the diaphragm during inspiration is known as paradoxical movement of the diaphragm and this condition is commonly seen in diaphragmatic palsy. The paradoxical movement of the ribs and the diaphragm, however, unrelatedly seems to have a common underlying physiology of negative intrathoracic pressure.
The external intercostals, the other inspiratory muscles, run in a downward and forward direction, starting from the inferior edge of the rib above and inserting into the superior margin of the rib below. The contraction of these muscles pulls the ribs upward and forward increasing both the lateral and anteroposterior diameters. The “bucket handle movement” of the rib brought about by these muscles is responsible for increasing the lateral diameter of the chest. These muscles receive innervation by the intercostal nerves coming off the spinal cord at the same level. The movement of the diaphragm and other inspiratory muscles results in negative intrathoracic pressure by the virtue of increased thoracic volume, whereas the contraction of the intercostals stabilizes the thoracic cavity and brings about a twisting movement. This action of intercostals makes the diaphragmatic activity more efficient and avoids wastage of energy. As the lungs are attached to the thorax by means of pleural membranes, the lungs also expand, creating a negative intrapleural and intrapulmonary pressure, thereby creating a rush of air to the lungs through the upper airway. Accessory muscles of respiration which include the scalene muscle (elevates the first and second ribs) and the sternomastoid which raises the sternum may be deployed in certain conditions like exercise, asthma, etc.
Expiratory Muscles
Expiration is almost always passive, mainly due to the natural elastic recoil of the lungs. Abdominal muscles like the rectus abdominis, internal and external oblique, transverses abdominis, and internal intercostals are a few of the expiratory muscles involved depending upon the clinical scenario.
One of the studies looking into biomechanics and mathematical calculations have demonstrated that local bending and shearing forces are the most important modes during an impact leading to rib fractures [12]. The bony thoracic cavity gets compressed under an external force in both the anteroposterior and lateral directions with the degree of damage depending upon the direction, the severity, and the surface area of the impact of the force. As seen already, the required force to produce a rib fracture in the pediatric population may have to be considerably higher due to the pliable nature of the ribs. If this force produces fracture of the rib at two points, a flail segment may occur. Paradoxical movement of the ribs should not be considered as an absolute diagnostic criterion, as the flail segment underlying scapular cover may not demonstrate paradoxical movement. Authors have also proposed two different terminologies, namely, flail segment and flail chest. Flail segment refers to a part of the chest wall that has detached from the adjacent thorax, whereas flail chest refers to clinical evidence of paradoxical motion [13, 14].
Based on the anatomical location, flail segment can be broadly defined into the following subcategories:
(a)
Anterolateral flail segment—the site of anterior fractures lies in the area of anterior rib angles.
(b)
Posterolateral flail segment—refers to those fractures where the posterior fracture comprises the posterior rib angle (Fig. 3.4).
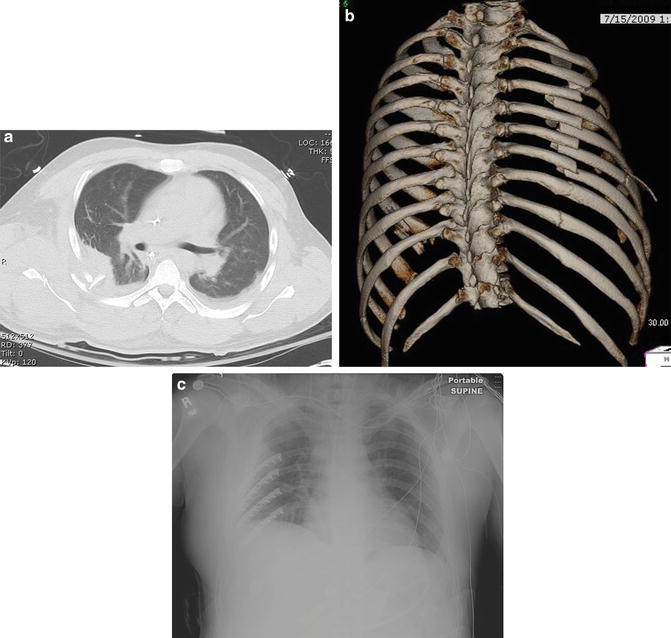
Fig. 3.4
A CT scan (a) of a severely displaced flail chest injury with multiple comminuted rib fractures and a localized hemothorax/pulmonary contusion. A 3D CT scan (b) provides excellent visualization of the injury, demonstrates the shortening and displacement of the posterior rib fractures, and aids in surgical planning. The patient was treated with early open reduction and plate fixation (c)
One important point to note, in both the above types of flail segment, is the involvement of the lateral segment, which is the site of insertion of serratus anterior muscles. Matteo in a series of studies in canine models [15–17] had demonstrated the role which respiratory muscles play following chest trauma in general and flail segment in particular. It would probably not be wrong to say that the term “floating segment” at times may not be observed clinically as these patients suffer from various other confounding variables like underlying pneumothorax, pulmonary contusion, and abdominal trauma. Normal mechanics of breathing are affected in the individuals suffering from flail chest due to various underlying conditions as stated above. Pain, which is one of the most common and most severe symptoms in this patient population, also alters the pattern of the respiratory muscle activation. In these canine model studies, they also note that the cranial movement of the fractured ribs was maintained during inspiration, with increased inspiratory activity recorded from the external intercostals by electromyography. They went on to prove that the respiratory displacement of the ribs is primarily determined by the balance between forces related to the fall in pleural pressure and that generated by the parasternal intercostal muscles. The extrapolation of the results from these animal studies to human subjects remains open to discussion, with further randomized trials on human subjects being warranted.
The altered role which the respiratory muscles play in this scenario is also very important. The serratus anterior with its digitations inserted on the ribs individually may act on each rib pulling it like an “arm on a drawer” leading to the dislocation of the ribs. This could also explain the tendency of the overriding ribs seen in flail segments following chest trauma.
Box 1 Anatomical Pearls [18]
Fracture of the First to Fourth Ribs
(a)
Involvement of the first rib is usually rare.
(b)
Fracture of the first three ribs usually indicates high-velocity trauma as they are well protected by the scapula from behind along with other associated musculatures.
(c)
(d)
The “surfer’s rib” is one typical example commonly seen in surfers performing layback maneuver where the first rib fracture may be noted [21].
Fracture of the Fifth to Ninth Ribs
(a)
They are usually more common and may be seen as an uncomplicated single rib fracture or may present with multiple fractures resulting in flail chest.
(b)
Inward displacement of the fractured ribs is associated with injury to the lung and other visceral organs.
Fracture of the 10th to 12th Ribs
Sternal Flail
A sternal flail chest is basically a form of anterior flail chest, where the flail segment is formed by the sternum, due to bilateral chondrosternal fracture. These fractures may be seen in the trauma resulting from frontal impact. Motor vehicle accident with steering wheel impact on the sternum is one of the most common causes leading to sternal fracture. Due to its anatomical location, the common associated injuries include pulmonary and cardiac contusion along with associated vascular injury. The presence of sternal fracture is however not indicative of cardiac contusion and does not warrant special investigation unless indicated otherwise [22].
Vertebral Flail
Support to the thoracic cage is provided by the spine posteriorly and sternum anteriorly. The three-column model of spine stability proposed by Denis was modified to a “4th spinal column” explaining the role of the sternum in providing stability to the thorax [23, 24]. High-velocity trauma sustained to the thorax could well be associated with traumatic vertebral injury. Involvement of the thoracic spine accounts for about 25–30 % of all spine fractures and is often seen following hyperflexion or axial loading and less commonly due to other mechanisms of injury [25]. Anterior wedge compression fractures and burst fractures are the most common types [20]. Multiple rib fractures coupled with sternal and/or vertebral fractures could lead to a complete bony disruption; however, fractures producing a flail segment of the spine are extremely rare and are mostly of academic interest.
Pathophysiology of Flail Chest and Thoracic Trauma
Thoracic trauma is one of the most common causes of trauma-related mortality and morbidity in both civilian and military life. The underlying injury and subsequent pathophysiology contributing to the fatalities and morbidity depend on the severity and the direction of the impact [26]. Single fractures of the ribs, therefore, are benign and are most often missed and, if at all diagnosed, pose few clinical difficulties. Liman and colleagues reviewed 1,490 patients admitted with chest trauma over a 2-year period and reported that the presence of two or more rib fractures is a marker of severe injury [26]. Eighty-one percent of these patients had hemothorax and/or pneumothorax at presentation. The mortality was also different with 0.2 % observed in patients without rib fractures and 4.7 in patients with more than two rib fractures. The detailed understanding of the pathophysiology is extremely important to help understand the difference in mortality and also effectively manage such a patient. The effect basically depends on the size of flail chest; however, the most important cause of respiratory compromise following flail chest is pulmonary contusion which is commonly seen in patients with an injury severity score (ISS) of more than 15. Various factors like direct blow, shearing or bursting at the gas-liquid interface and high- and low-density interface, and transmission of shock waves play a role in the causation of pulmonary contusion either alone or in combination.
The main factors leading to serious morbidity in patients with rib fractures are respiratory insufficiency due to pain, underlying lung collapse, paradoxical movement, and underlying pulmonary contusion. Of all the above, pulmonary contusion is the most important, along with the fall in total lung capacity and functional residual capacity due to paradoxical motion, which contributes to hypoxia. Other factors which could also contribute to hypoxia in these patients could be injury primarily to the pleura and lung such as pneumothorax and aspiration or secondary to brain injury or cardiac injury. Table 3.1 enumerates a few important life-threatening events which could be encountered in patients presenting with thoracic trauma and multiple rib fractures that are flail.
Table 3.1
Life-threatening complications following thoracic trauma
Immediate threats to life | Potential threats (not immediate) |
|---|---|
1. Tension pneumothorax 2. Cardiac tamponade 3. Airway obstruction 4. Major vascular tear | 1. Pulmonary and myocardial contusion 2. Vascular disruption 3. Flail chest 4. Diaphragmatic and esophageal rupture |
In earlier days, the pulmonary contusion was not well recognized, and its clinical relevance was never emphasized until World War I, where a number of soldiers were noticed to have died without suffering obvious external trauma [27]. Paradoxical motion of the chest wall was also considered to be the main cause of respiratory embarrassment in this subset of patients. This “pendelluft” or out-of-phase movement of the chest wall refers to the to-and-fro movement of deoxygenated air between the lung of the normal and flail side during spontaneous breathing and was considered to be the main cause of respiratory insufficiency. However, certain canine-based studies later refuted this hypothesis. Now, it is widely believed and accepted that it is the underlying pulmonary contusion (PC) which is the major cause of the poor prognosis following a flail chest along with rib fractures causing secondary problems of pain and muscular splinting (Fig. 3.5). Fulton in an animal study also concluded that PC is mainly a progressive condition starting with parenchymal injury worsening over the initial 24 h [28].
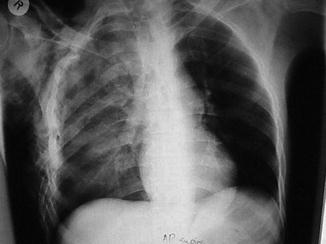
Fig. 3.5
Chest radiograph with a right-sided flail chest injury: multiple segmental rib fractures and a pulmonary contusion are evident
The pathophysiology of pulmonary contusion (PC) is still not fully understood, but primarily involves alveolar and capillary wall rupture leading to intra-alveolar hemorrhage and flooding resulting in ventilation-perfusion (V/Q) mismatch and subsequent hypoxia. The area of PC is often localized to the area adjacent to rib fractures (Fig. 3.6). These patients often tend to develop type 1 respiratory failure due to underlying ventilation-perfusion mismatch and arteriovenous shunting.
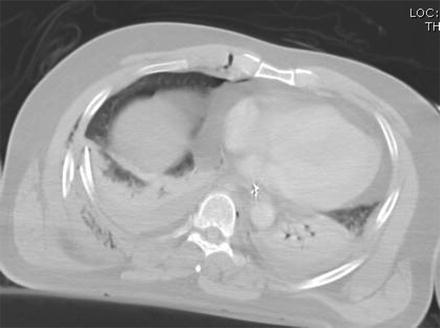
Fig. 3.6




This CT scan demonstrates how the area of pulmonary contusion is typically adjacent to the area of greatest deformation of the injury to the ribs or chest wall, in this case near the posterior fractures of the lower right ribs (case courtesy of W. Drew Fielder, MD, FACS)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
