Cine Gradient Echo Imaging
Spin echo imaging is the “meat and potatoes” of cardiac MRI and used for evaluation of anatomy. Cine gradient recalled echo (GRE) imaging adds the spice of functional imaging. With cine GRE, the same slice is imaged at multiple time points in the cardiac cycle. The multiple frames are viewed in a cinematic loop (hence, the term cine). The movie gives the viewer an appreciation for flow and function in the heart and vessels. For example, whereas a routine MR angiogram may depict ascending aortic pathology, cine imaging provides the functional assessment of the aorta and aortic valve. In emergency cases, cine GRE may help distinguish between aortic dissection and intramural hematoma by demonstrating flow in the false lumen.
Like ECG-gated spin echo imaging, cine GRE is performed using ECG-gating. Data for each image are acquired across several heartbeats. Compared to spin echo methods, cine GRE pulse sequences are more complex, because they require that several additional parameters be adapted to the subject’s heart rate and breath-holding capabilities. The aim of this chapter is to clarify the challenges of optimizing cine GRE.
KEY CONCEPTS
[right half black circle] Cine gradient echo acquisitions rely on robust and consistent ECG gating.
[right half black circle] Acquisition times are usually defined in terms of number of heartbeats (rather than in absolute units of time).
[right half black circle] Temporal resolution and spatial resolution must be balanced against acquisition time.
[right half black circle] Retrospective gating allows reconstruction of images throughout the cardiac cycle, whereas prospective gating typically excludes late diastole.
[right half black circle] Image contrast depends on whether spoiled gradient echo or steady-state free precession gradient echo sequences are performed.
[right half black circle] Segmented k-space sequences allow the user to vary temporal resolution of images; increased temporal resolution comes at the expense of either decreased spatial resolution or increased acquisition time.
[right half black circle] View sharing increases the apparent temporal resolution of a cine gradient echo sequence without increasing acquisition time.
[right half black circle] Steady-state free precession sequences have sufficient signal-to-noise ratio to warrant routine implementation with parallel imaging methods.
[right half black circle] Accurate quantification of functional parameters such as left ventricular ejection fraction requires careful attention to the demarcation of blood pool at end systole and end diastole.
[right half black circle] Pitfalls of cine gradient echo imaging may relate to inaccurate ECG gating, poor image contrast, and flow-related signal loss, among others.
[right half black circle] Clinical Protocol:
[right half black circle] Left ventricular function
PRINCIPLES OF CINE GRE
Before delving into the details of specific types of cine GRE sequences, it is necessary to review some themes common to all cine GRE techniques. These include the definition of temporal resolution, segmented k-space methods, partitioning of MR data into frames, and image contrast.
Cine GRE relies on ECG-gating for an accurate representation of cardiac motion. It may be helpful for the reader to review Chapter III-1 on the electrocardiogram (ECG) and the basics of ECG gating. An understanding of the concepts of trigger delay, acquisition window, trigger window, R-R interval, and prospective versus retrospective gating (Figure III1-2 and III1-10) is assumed.
IMPORTANT CONCEPT:
As with all ECG-gated sequences, the most critical step for successful imaging is placement of ECG leads and confirming a good ECG tracing for gated sequences (see Chapter III-1).
Number of Frames and Temporal Resolution
With cine GRE, multiple images at the same slice position are generated to capture different time points in the cardiac cycle. The terminology to describe these images can be confusing. For clarity, the individual images are referred to as frames, rather than “cardiac phases” (Figure III4-1).
The multiple frames of a cine GRE sequence are played in a cinematic loop to show a video of the beating heart. The temporal resolution and number of frames define how smooth or jerky the cine loop appears. The temporal resolution of the cine GRE acquisition is usually defined as the duration of the cardiac cycle that each frame represents. For example, if each frame is acquired in 50 msec intervals after the R wave, then the temporal resolution is 50 msec. If MR data are acquired for 700 msec of each heart beat, then the number of frames will be 14. Higher-temporal-resolution images are needed for more accurate assessment of cardiac motion and function, particularly during systole. As will be discussed later in this chapter, some images can be generated by interpolation (view sharing or echo sharing in k-space). The true temporal resolution of interpolated data is more complicated to determine.
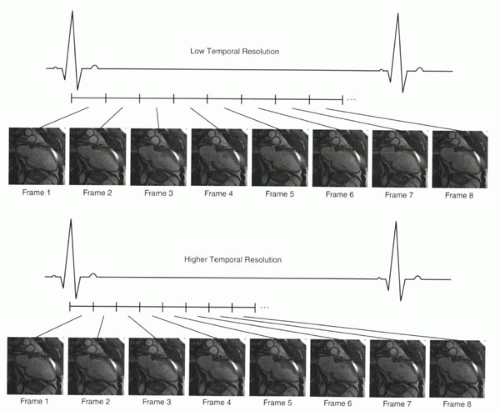 FIGURE III4-1. Low- versus higher-temporal-resolution prospectively gated cine gradient echo acquisition. The eight low-temporal-resolution images sample fewer time points across the cardiac cycle. The first eight frames of the higher-temporal-resolution images better reflect cardiac motion during systole, when dyskinesis of the thinned apex can be seen. Recall that with prospectively triggered sequences, images of the heart immediately preceding the R wave are not obtained. |
ECG-Gated Data: Sorting into k-Space Frames
ECG-gated sequences acquire gradient echoes repeatedly after each R wave for the entire duration of the acquisition window. The manner in which the echoes are partitioned or segmented into different k-spaces determines the temporal resolution of the images and also the total acquisition time. Each k-space corresponds on a one-to-one basis to a specific frame (Figure III4-2). Generally, only a small proportion of the data needed to fill each k-space is collected in a single heartbeat. The amount of data needed to fill each k-space determines the spatial resolution of the images (the number of phase-encoding steps). The number of heartbeats needed to fill a given k-space determines the total acquisition time for the sequence.
Because the k-space data for each frame are collected across a number of heartbeats, the image quality is strongly dependent on the consistency of cardiac motion and gating from beat to beat.
CHALLENGE QUESTION: You run a prospectively triggered sequence and listen to the sounds of the system. The rhythm is irregular. At first there is a run of three bursts at about one every second, but then there is a pause, a couple more bursts, and then more pauses. What is happening, and how can you solve this problem?
View Answer
Answer: While a prospectively ECG-triggered sequence is running, the noises emanating from the scanner should be rhythmic, one burst per heartbeat. If the noises are erratic, then either the subject’s heart rate is irregular or the triggering is not working properly. If it seems that the machine is skipping beats, the problem may lie in the acquisition window being too long relative to the R-R interval (Figure III4-3). Reducing the acquisition window to 80% of the R-R interval (or increasing the trigger window to 20%) may solve the problem. Another important factor to check is whether the heart rate of the subject is changing during a breath-hold acquisition. The acquisition window should be based on the R-R interval during breath holding.
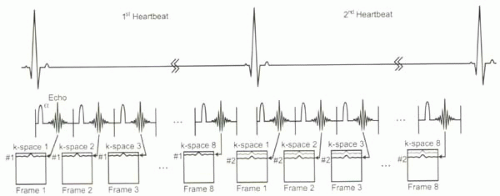 FIGURE III4-2. k-space filling for the multiple frames of an ECG-gated cine gradient echo sequence. In this example, with each heartbeat, one line of k-space is collected for each frame. The total number of heartbeats needed to fill all k-spaces equals the number of phase-encoding steps for each image. For example, if NPE = 100, then the acquisition time will be 100 heartbeats. |
The quality of ECG-gated images, particularly cine GRE images, relies not only on having a reasonable temporal resolution, but also, importantly, on the consistency of data acquisition with respect to the ECG. For example, the MR system assumes that the cardiac position immediately after the R-wave is the same for all heartbeats. Therefore, when echoes are acquired at this time point over multiple beats, the resulting image should be a perfect representation of the heart at that point in time. The system similarly assumes that the heart position at, for example, 240 msec and 560 msec after the R wave is the same from beat to beat as well. However, with irregular rates or premature beats, this may not be true (Figure III4-3). Combining data that reflects the heart in different states of contraction will degrade image quality substantially.
CHALLENGE QUESTION: What other consequences of poor ECG gating could lead to image degradation?
View Answer
Answer: Poor ECG gating may also result in many heartbeats where no data is collected (Figure III4-3, fourth heartbeat). An occasional missed R-wave will not degrade image quality substantially. But if this happens often, then the total acquisition time will exceed the breath hold, causing motion artifacts and further reducing image quality.
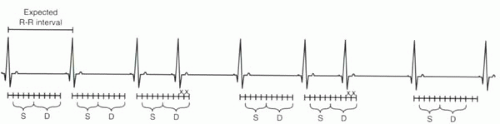 FIGURE III4-3. Effect of irregular heart rate on acquisitions when R-R intervals are shorter than expected. The “x” labels denote data that are presumed to reflect diastole (D) but that in fact correspond to early systole (S). |
IMPORTANT CONCEPT:
Reliable ECG-gating and regular heart rates are necessary for images to reflect cardiac motion accurately.
Acquisition Time
For cardiac MR pulse sequences, acquisition times are usually a multiple of heartbeats rather than of seconds. The acquisition times therefore depend on a subject’s heart rate. Because most cardiac MR examinations require cine acquisitions in multiple planes of the heart, it is vital that cine gradient echo acquisition times be short enough for a comfortable breath hold. A subject’s breath-holding capacity is usually thought of in seconds (and not heartbeats!). Most healthy individuals can suspend respiration for 20 sec. Those with moderate cardiac or respiratory ailments are usually still able to hold their breath for 10 sec, particularly if supplemented with oxygen via nasal cannula. If acquisition times exceed the breath-holding capacity of subjects, then the ECG-gated images should be performed during free breathing with 3-4 signals averaged, thereby lengthening the acquisition times by a factor of 3-4.
IMPORTANT CONCEPT:
With ECG-gated cine GRE sequences, acquisition times are better thought of in terms of number of heart beats rather than in absolute time (seconds). Sequences with acquisition times that exceed a subject’s capacity for breath holding (despite supplementary oxygen) may need to be performed with multiple signal averages during free breathing.
Tradeoffs: Temporal Resolution vs Spatial Resolution vs Acquisition Time
For all cine GRE images, acquisition parameters can be modified to balance the tradeoffs between temporal resolution, spatial resolution, and acquisition times (Figure III4-4). Fundamentally, the parameter that constrains all three is the minimum time needed to generate each gradient echo, reflected in the minimum TR, and this varies depending on the MR system and the pulse sequence used.
In general, ideal temporal resolution of sequences performed for assessment of cardiac function should be 50-60 msec or less, depending on the subject’s heart rate. The faster the heart rate, the better the temporal resolution needed to resolve the motion of the heart during systole. If temporal resolution is inadequate, the cine images are likely to underestimate left ventricular contractility.
The spatial resolution of cine GRE images depends on the structures that need to be resolved. For studies of overall cardiac function, an in-plane spatial resolution of 2-2.5 mm is probably sufficient. Higher spatial resolution, such as 1-2 mm, helps to define finer structures such as cardiac valves, a patent foramen ovale, or smaller vessels such as coronary arteries or bypass grafts. Typical imaging fields of view are about 250 mm × 350 mm (allowing for rectangular field of view for short axis views). Thus for a standard 100-128 × 256 matrix, the in-plane spatial resolution is usually approximately 2-2.5 mm × 1.4 mm. A 192 × 256 matrix provides superior resolution of 1.3 × 1.4 mm.
CHALLENGE QUESTION: What are the drawbacks of setting TR to a minimum?
View Answer
Answer: Recall from Chapter I-8 that one of the main ways to reduce TR is by using a higher receiver bandwidth. Higher-bandwidth sequences result in lower signal-to-noise ratios. Therefore, there are limits to how low TR can go without sacrificing image signal. Also, as will be discussed subsequently, with spoiled gradient echo sequences, short TRs will reduce the contrast between blood pool and myocardium.
Most vendors preset sequences with a minimum TR based on the desired image quality and contrast of a sequence. After TR is fixed, the next consideration in setting up a cine GRE sequence is usually the acquisition time, constrained by the subject’s breath-holding capacity. For a given TR and acquisition time, parameters of a cine GRE sequence are selected based on the desired balance between spatial and temporal resolution (Figure III4-4).
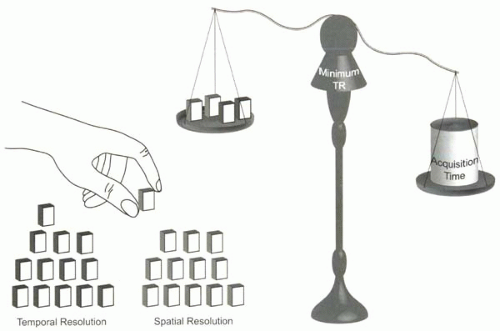 FIGURE III4-4. The balance between spatial resolution, temporal resolution, and acquisition time. For a given minimum TR, acquisition time depends on the spatial and temporal resolution. To keep acquisition time constant (with a given minimum TR), there must be a proper compromise between spatial and temporal resolution. |
IMPORTANT CONCEPTS:
Image acquisition parameters, guided by the minimum TR for the sequence, are based on the trade-offs between temporal resolution, spatial resolution, and acquisition times. Ideally, acquisition times should be less than 15-20 sec to accommodate breath holding. Temporal resolution should be 50-60 msec or less. Spatial resolution should be 2-2.5 mm or less.
Image Contrast
Cine GRE sequences are designed to evaluate flow and function of the myocardium and vessels. They are typically referred to as bright-blood sequences, because the signal intensity of the blood is bright relative the myocardium and vessel wall. How this image contrast is achieved varies with the type of pulse sequence. With standard spoiled gradient echo sequences, the image contrast is based on the time-of-flight phenomenon, similar to that discussed in Chapter II-2. Repeated RF pulses cause saturation of the stationary tissues, while the inflow of fresh, unsaturated protons in moving blood leads to its relatively high signal intensity. To allow time for the inflow of moving blood, the TR of these gradient sequences is on the order of 8 msec or more. Even with a TR of 8 msec, if blood flow is slow, signal of the blood pool can become saturated and the contrast between myocardium and blood pool reduced.
Because of the need to allow time for inflow, these sequences are not able to take advantage of the ultrashort TRs possible with newer MR systems. Steady-state free precession sequences, as described in Chapter I-4, produce images with high contrast between blood and myocardium based on their T2 (and T1) differences (Figure I4-19), independent of flow. These sequences benefit from shorter TRs and TEs, which in turn translate into shorter acquisition times or higher-spatial-resolution images in equivalent acquisition times.
More details about the different methods used to produce cine GRE images are outlined in the following sections and summarized in Table III4-1.
[right half black circle] TABLE III4-1 Cine Gradient Echo Pulse Sequence Options | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
CONVENTIONAL ECG-GATED CINE GRE: BASIC VERSION
A standard ECG-gated cine GRE sequence is available for cardiac imaging on almost all 1.5-3 T MR systems. With the standard spoiled gradient echo sequence, only one echo is collected for each k-space during a given heartbeat (Figure III4-2). Depending on the number of phase-encoding steps, the total acquisition time is between 100 and 128 heartbeats, or about 2 min. Because 2 min is too long for a breath hold, respiratory motion will degrade these acquisitions unless multiple signal averages are performed. With 3-4 signal averages, about 5-8 min are required for one cine loop of a single slice position.
Choosing Parameters for Imaging
With conventional cine GRE, the temporal resolution is equal to the TR for the sequence. TR is usually about 50-60 msec, so that 10-15 frames are produced. The flip angle is selected based on image contrast and the TR. A typical flip angle of 15-20° gives a good balance between the amount of signal in the image and the image contrast between blood and myocardium. Because the image acquisition time is directly proportional to the number of phase-encoding steps, rectangular field of view is valuable for reducing acquisition times without sacrificing spatial resolution.
IMPORTANT CONCEPT:
Using the basic cine GRE sequence, the minimum TR and TE should be used with a flip angle of about 20°. To reduce motion artifacts, 3-4 signal averages result in a total acquisition time of approximately 5-8 min per slice position.
SEGMENTED k-SPACE CINE GRE
With stronger gradients and faster slew rates, gradient echoes can be generated in 10 msec or less. Then, in the same time that a conventional cine GRE sequence takes to acquire one line of k-space, the faster sequence can acquire say, 5. Each consecutive set of 5 echoes is used to fill the k-space of the corresponing frame (Figure III4-5). To fill each k-space completely, the number of heart beats required is reduced by a factor of 5. For example, for images with a matrix of 100 × 256, the acquisition time would be reduced from 100 heartbeats (for each signal or excitation) to 20 heartbeats. This difference is critical, because now the acquisition time is short enough for a single breath hold; multiple signal averaging is no longer necessary.
The acquisition of multiple lines of k-space in a given heartbeat is referred to as segmented k-space cine gradient echo imaging.
The terminology for the TR of segmented k-space sequences can be confusing. For clarity, the following terms and definitions will be used in the remainder of this book:
TR: Although, strictly speaking, the TR should be defined as the time between consecutive RF pulses, with cine GRE imaging the TR is usually used to refer to the temporal resolution. In the foregoing example, the “TR” would be 50 msec.
True TR: This separate term will be used to specify the actual time between consecutive RF pulses. In the example, the “true TR” would be 10 msec.
Views per segment (vps) or Lines per segment: The number of gradient echoes acquired for each frame during a single heartbeat. In the example, the views per segment would be 5. The TR is equal to the true TR multiplied by the vps. Examples of different numbers of views per segment are illustrated in Figure III4-5.
Choosing Parameters for Cine GRE
The choice of views per segment offers an additional flexibility in planning a cine GRE acquisition. It is selected based on the desired relationship between spatial
resolution, temporal resolution, and acquisition time. Typically, a temporal resolution of 50-60 msec is desired, corresponding to about 10-15 frames. If temporal resolution is too low (for example, if only 6-8 frames are acquired at 100 msec intervals), then the information about the heart’s motion might be inadequate for interpretation. To show fine detail such as cardiac valves, ideally, the spatial resolution should be less than 2 mm. Finally, acquisition time is usually kept less than 20 sec for breath holding. With ECG-gated sequences, acquisition time depends on number of heartbeats, and so the actual acquisition time depends on the subject’s heart rate.
resolution, temporal resolution, and acquisition time. Typically, a temporal resolution of 50-60 msec is desired, corresponding to about 10-15 frames. If temporal resolution is too low (for example, if only 6-8 frames are acquired at 100 msec intervals), then the information about the heart’s motion might be inadequate for interpretation. To show fine detail such as cardiac valves, ideally, the spatial resolution should be less than 2 mm. Finally, acquisition time is usually kept less than 20 sec for breath holding. With ECG-gated sequences, acquisition time depends on number of heartbeats, and so the actual acquisition time depends on the subject’s heart rate.
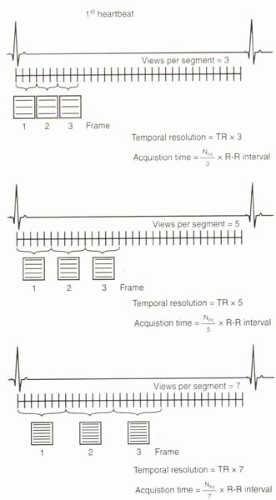 FIGURE III4-5. Segmented k-space cine gradient echo sequences shown with 3, 5, and 7 views per segment. The more views per segment, the shorter the acquisition time at the cost of worsening temporal resolution. |
Given the interplay of these parameters, how should a sequence be set up based on a subject’s heart rate and breath-holding capacity?
Consider the following two sample subjects: one with a heart rate of 60 beats per minute (A) and another with a heart rate of 90 beats per minute (B). In both cases, the same sequence is used—a prospectively gated segmented k-space cine GRE sequence with true TR = 10 msec. The desired imaging matrix for an axial view is 100 × 256 (assuming recFOV is used). What is the relationship between temporal resolution and acquisition time in these two cases when views per segment is varied?
Case A: Heart Rate of 60 Beats per Minute
In this subject, the R-R interval is 1 sec or 1000 msec. The use of prospective gating means that the usable period of the R-R interval for data acquisition is reduced to about 85% of the R-R interval, or 850 msec. Within this time, for a TR of 10 msec, a total of up to about 85 echoes can be generated. How these echoes are allocated to different k-spaces depends on the vps (Figure III4-6).
Scenario A-1 (Figure III4-6, Case A): vps = 5
If each consecutive set of 5 echoes is assigned to a separate k-space frame, then the temporal resolution of the cine images will be 50 msec. With this temporal resolution, a total of 17 frames (850/50) will be generated. Twenty heartbeats will be needed to fill each k-space with 100 echoes (100 phase-encoding steps). With a heart rate of 60 beats per minute, the acquisition time will be 20 sec, assuming perfect triggering.
Scenario A-2 (Figure III4-6, Case A): vps = 7
If each consecutive set of 7 echoes is assigned to a separate k-space frame, then the temporal resolution of the cine images will be 70 msec




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
