Ventricular Septal Defect
A ventricular septal defect can occur as an isolated lesion or in combination with other anomalies.
Surgical Anatomy
The embryologic development of ventricular septal defects is interesting and has been the basis for many complex classifications. We prefer a classification proposed by Anderson, which is simple and has many clinical implications, particularly from the surgeon’s point of view. Anderson divides ventricular septal defects into perimembranous, subarterial-infundibular, and muscular types.
The perimembranous variety of ventricular septal defects encompasses subgroups of defects that occur near the membranous segment of the interventricular septum and includes those septal defects commonly seen in tetralogy of Fallot and atrioventricular septal defects (Fig. 21-1). Because the path of the conduction tissue is intimately related to the inferior rim of these defects, an accurate knowledge of the surgical anatomy of this region is most helpful.
The atrioventricular node is situated in its usual position at the apex of the triangle of Koch, whose boundaries consist of the septal attachment of the tricuspid valve, tendon of Todaro, and the coronary sinus as its base (Fig. 21-2). The conduction tissue passes from the atrioventricular node as the bundle of His through the central fibrous body and the tricuspid annulus into the ventricular septum, following a course along the inferior rim of the defect toward the left ventricular side of the septum.
Surgical Approach
All forms of ventricular septal defects are approached through a median sternotomy.
Cannulation
Cardiopulmonary bypass with moderate systemic hypothermia is used in most patients. In very small infants (<2 kg), deep hypothermic arrest using a single venous cannula through the right atrial appendage for cooling and warming may be preferred. In all others, the superior vena cava is cannulated directly; similarly, the inferior vena cava is cannulated through the atrial wall just above the origin of the inferior vena cava (see Chapter 2). Tapes are then passed around both cavae.
Myocardial Preservation
Cardioplegic arrest of the myocardium is maintained by intermittent infusion of cold blood cardioplegia into the aortic root (see Chapter 3).
Transatrial Approach to a Ventricular Septal Defect
Almost all the perimembranous and atrioventricular canal types of ventricular septal defects and many of the muscular variety can be exposed and closed through the right atrium. The subarterial-infundibular type is best approached through a limited right ventriculotomy or preferably a pulmonary arteriotomy.
The aorta is cross-clamped, and cardioplegic solution is administered into the aortic root. The venae caval snares are then snugged down. A longitudinal or oblique atriotomy is made, starting at a point 0.5 to 1 cm anterior and parallel to the sulcus terminalis, and is extended toward the orifice of the inferior vena cava. The edges of the incision are then retracted to provide a good exposure of the tricuspid valve and the triangle of Koch (Fig. 21-3).
If a patent ductus arteriosus is present, it should be occluded with a metal clip before the initiation of cardiopulmonary bypass to prevent pulmonary overcirculation and suboptimal systemic perfusion (see Chapter 14).
The sinoatrial node is vulnerable to injury from the snare around the superior vena cava. It can also be injured if the atriotomy is extended too far superiorly.
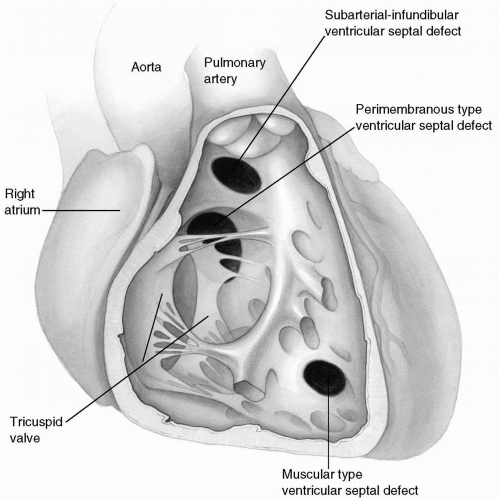 FIG 21-1. Types of ventricular septal defects. |
 FIG 21-2. Surgical anatomy of the right atrium. |
 FIG 21-3. Exposure of a ventricular septal defect by retracting the tricuspid valve leaflets. |
Technique for Closure
The anterior leaflet of the tricuspid valve is retracted with a 6-0 Prolene suture or small vein retractor to expose the defect and its margins for identification (Fig. 21-3). The defect can be closed with a continuous suture technique using 5-0 Prolene, or multiple interrupted sutures of 4-0 or 5-0 braided sutures buttressed with Teflon felt pledgets, or a combination thereof.
Continuous Suture Technique
With a double-armed, half-circle needle of 5-0 Prolene, the suturing is started at the 12 o’clock position along the muscular rim. The needle is then passed through a patch of Dacron velour slightly larger in size than the defect, again through the muscular rim, and then again through the patch, which is subsequently lowered into position (Fig. 21-4).
The suturing is continued in a counterclockwise direction along the superior rim, which overlies the aortic valve, until the central fibrous junction of the septum, aortic root, and tricuspid annulus is reached. The needle is passed through the septal leaflet of the tricuspid valve. During the procedure, the placement of each stitch is facilitated by the assistant applying slight traction on the Prolene suture.
 FIG 21-4. Patch closure of a ventricular septal defect using a continuous suture technique. |
Occasionally, the muscular rim of the ventriculoseptal defect may be very friable, allowing the fine Prolene to cut through. This is more likely to happen when there is associated long-standing muscular hypertrophy, as in tetralogy of Fallot. Multiple interrupted sutures buttressed with pledgets are then substituted for the continuous suture technique (Fig. 21-5).
The aortic valve leaflets are immediately below the superior margin of the defect and can be punctured during suturing if deep needle bites are taken in this area (Fig. 21-6).
The junction of the tricuspid annulus, aortic root, and septum is a vulnerable area where a residual defect may occur. A transitional stitch incorporating the tricuspid leaflet, the rim of the defect, and the patch will ensure a more secure closure (Fig. 21-7). This can be satisfactorily accomplished with either an interrupted or a continuous suturing technique.
The other arm of the Prolene suture is then continued in a clockwise direction; superficial bites that include only endocardium are taken along the inferior rim of
the defect, until the tricuspid leaflet is reached (Fig. 21-7). Alternatively, the other arm of the suture is continued, moving outward to a distance of 3 to 5 mm from the rim of the defect to avoid the underlying conduction tissue (Fig. 21-8).
the defect, until the tricuspid leaflet is reached (Fig. 21-7). Alternatively, the other arm of the suture is continued, moving outward to a distance of 3 to 5 mm from the rim of the defect to avoid the underlying conduction tissue (Fig. 21-8).
 FIG 21-5. Interrupted suture technique for closure of a ventricular septal defect. |
 FIG 21-6. Proximity of an aortic valve leaflet to the rim of the septal defect. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


