Left Ventricular Outflow Tract Obstruction
Congenital Aortic Stenosis
Pathologic findings in congenital aortic stenosis can vary. The valve may be bicuspid, tricuspid, or unicuspid, and the commissures may be fused together in any combination. The functional orifice of the aortic valve, however, is usually between the left and noncoronary cusps, whereas the other cusp and commissures are fused and deformed to various degrees.
Infants or neonates with critical aortic stenosis may require urgent intervention. Neonates may present in extremis with marked metabolic acidosis. Infusion of prostaglandin E1 may improve the circulation in these neonates by reopening the ductus arteriosus. It is critical in these cases to differentiate isolated, critical aortic stenosis from a form of hypoplastic left heart syndrome that requires a modified Norwood procedure (see Chapter 30). Although percutaneous balloon valvuloplasty for critical aortic stenosis in the neonate and infant is being performed with satisfactory results, surgery is still indicated for some patients.
Valvotomy Technique
A median sternotomy approach is used. Surgical valvotomy is performed on cardiopulmonary bypass. Cannulation is carried out with a standard aortic cannula and a single venous cannula in the right atrial appendage. Cardiopulmonary bypass is begun, and the ductus arteriosus is closed with a heavy tie or metal clip. The aorta is cross-clamped, and cardioplegic solution is administered (see Chapter 3). The aorta is incised transversely, the aortic valve is exposed, and its anatomy is studied closely. A no. 15 blade is used to incise the fused commissures to within 2 mm of the aortic annulus (Fig. 24-1).
The purpose of the surgery is to relieve obstruction to the left ventricular outflow tract in these very sick infants as effectively as possible, without producing aortic insufficiency. Therefore, overzealous incision of the commissures or division of a rudimentary raphe only results in gross aortic insufficiency and may necessitate aortic valve replacement (Fig. 24-2).
Conversely, inadequate relief of the obstruction may not help the child very much. Experience provides the good judgment required to incise to just the right extent at the precise area of a grossly deformed aortic valve.
When the aorta is small, an oblique rather than transverse aortotomy provides better exposure of the aortic valve.
It is of paramount importance to inspect the aortic subvalvular area and rule out the presence of a fibrous diaphragm or other forms of left ventricular outflow tract obstruction. A Hegar dilator of appropriate size can be used for precise evaluation of the valvular orifice and the left ventricular outflow tract.
A satisfactory commissurotomy with long-lasting good results depends on how well the valve was formed initially. When there is severe deformity and maldevelopment of the aortic valve, surgical relief of left ventricular outflow tract obstruction is only temporary and palliative. These subgroups of patients should be followed closely so that a more definitive form of treatment can be performed before permanent left ventricular dysfunction ensues.
Resection of the Subvalvular Diaphragm
A fibrous, muscular, or membranous rim of tissue arising from the anterior two-thirds of the left ventricular outflow tract may be present within 1 cm below the aortic annulus. The aortic valve leaflets are retracted gently with narrow ribbon retractors. The fibromuscular diaphragm is then excised with a no. 15 blade (Fig. 24-3A, B). This shelf of
abnormal tissue can also be mobilized and enucleated in its whole circumference with an endarterectomy spatula.
abnormal tissue can also be mobilized and enucleated in its whole circumference with an endarterectomy spatula.
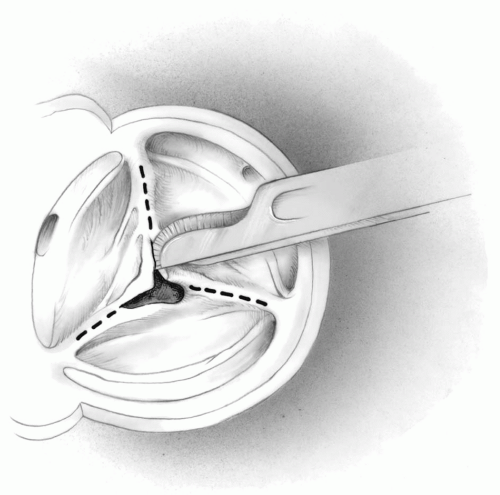 FIG 24-1. Technique for aortic commissurotomy. |
A myotomy or a limited myectomy involving the bulging septum is recommended to prevent the possible persistence of a significant residual obstruction (Fig. 24-3C). This may also help to prevent recurrence of the membrane, the incidence of which is higher the younger the patient is when the initial surgery is performed.
A substantial segment of the abnormal fibromuscular tissue can be excised and removed from the septal area without producing a defect in the interventricular septum. If such a complication does occur, the defect must be identified and closed. Pledgeted sutures are essential to protect the friable muscular tissue.
 FIG 24-2. Overzealous incision of the commissures, causing aortic insufficiency. |
Only the white fibrous tissue should be mobilized and removed from the area immediately below the rightward half of the right cusp and the commissure between the right and noncoronary cusps. Otherwise, the conduction tissue may be injured resulting in heart block (Fig. 24-3B).
Occasionally, the membranous tissue is adherent to the underside of the right coronary leaflet of the aortic valve. It must then be meticulously dissected free without damaging the aortic valve to avoid producing valvular insufficiency.
Occasionally, the lesion may extend and become adherent to the anterior leaflet of the mitral valve; in this case, it should be dissected free with the utmost care. Injury to the mitral valve near its annulus may result in an opening into the left atrium.
Hypertrophic Obstructive Cardiomyopathy
Hypertrophic obstructive cardiomyopathy is usually not a surgical lesion. Many patients respond to β-blockers or calcium channel blockers. Dual-chamber cardiac pacemakers may be useful in some patients. For severely symptomatic patients, ventricular septal myectomy is an established treatment. A relatively thick segment (1-cm deep by 1.5-cm wide) of septal wall extending downwards to the base of the papillary muscles is excised and removed (Fig. 24-4).
Most surgeons use a transaortic approach. Exposure is facilitated by extending the aortotomy obliquely down to the noncoronary annulus and placing plegeted sutures just above the valve commissures. By placing traction on these sutures, the hypertrophied septum can be visualized. After the initial wedge resection, a small rake retractor can be placed into the septum and pulled upwards toward the aortic annulus to allow visualization and resection of the apical portion of the septum.
When systolic anterior motion of the anterior leaflet of the mitral valve is a significant component of the
left ventricular outflow tract obstruction, an adequate septal myectomy usually resolves the abnormal motion of the anterior leaflet and any mitral regurgitation. However, some patients have associated abnormalities of the mitral subvalvular apparatus, which must be recognized and treated at the time of surgery. These include anomalous papillary muscle insertion directly into the anterior leaflet of the mitral valve and abnormal chordae tendineae attaching to the ventricular septum. If present, the abnormal chords are resected, and any areas of fusion of the papillary muscle(s) to the septum or free wall are divided. Occasionally, a valvuloplasty procedure to shift the coaptation level of the valve posteriorly may be required. This may involve anterior and/or posterior leaflet plication usually combined with an annuloplasty. A simple technique that may be effective is an Alfieri stitch placed 1 cm away from the free edges connecting the central portion of the anterior and posterior leaflets (see Chapter 6). Rarely, the mitral valve must be replaced with a low-profile prosthesis, resecting the entire anterior subvalvular apparatus. When combined with a myectomy, these techniques result in relief of the obstruction.
left ventricular outflow tract obstruction, an adequate septal myectomy usually resolves the abnormal motion of the anterior leaflet and any mitral regurgitation. However, some patients have associated abnormalities of the mitral subvalvular apparatus, which must be recognized and treated at the time of surgery. These include anomalous papillary muscle insertion directly into the anterior leaflet of the mitral valve and abnormal chordae tendineae attaching to the ventricular septum. If present, the abnormal chords are resected, and any areas of fusion of the papillary muscle(s) to the septum or free wall are divided. Occasionally, a valvuloplasty procedure to shift the coaptation level of the valve posteriorly may be required. This may involve anterior and/or posterior leaflet plication usually combined with an annuloplasty. A simple technique that may be effective is an Alfieri stitch placed 1 cm away from the free edges connecting the central portion of the anterior and posterior leaflets (see Chapter 6). Rarely, the mitral valve must be replaced with a low-profile prosthesis, resecting the entire anterior subvalvular apparatus. When combined with a myectomy, these techniques result in relief of the obstruction.
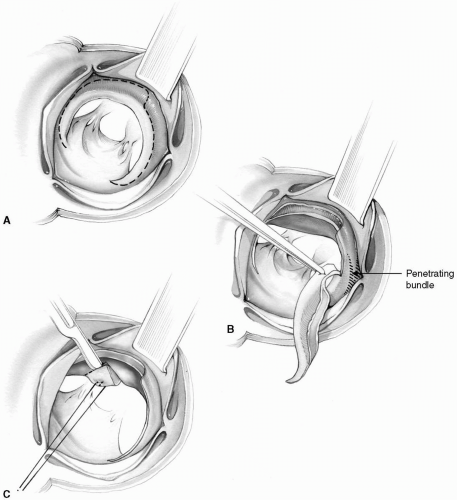 FIG 24-3. Resection of a subvalvular diaphragm. A: Dashed line depicts the extent of resection. B: Only the white fibrous tissue is resected near the penetrating bundle. C: As an extra precaution against inadequate relief of an obstruction, a limited myectomy is also carried out. |
All anomalous chords attached to the free edge of the anterior leaflet must be preserved to prevent a flail leaflet.
During the process of excising the hypertrophied muscle, fragments may fall into the left ventricular cavity, resulting in a subsequent embolism. This can be prevented to some degree by pulling on the desired segment to be excised with a 4- 0 or 5-0 Prolene stitch (Fig. 24-4). A biopsy forceps may be used to resect muscle from the more apical portions of the septum. Care should be taken to remove all debris from within the left ventricular cavity.
Exposure may be inadequate through the retracted aortic leaflets. The obstructing muscle may then be removed through a left atriotomy working through the mitral valve.
Recently, a catheter technique that injects pure alcohol into a septal perforator artery has been used successfully to produce an infarction of the septum and lower the gradient across the left ventricular outflow tract. The role of this procedure needs to be further delineated.
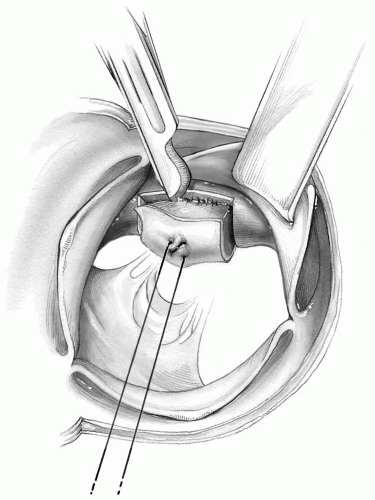 FIG 24-4. Myectomy for idiopathic hypertrophic subaortic stenosis. Two longitudinal incisions, one below the commissure between the left and right leaflets and the other below the nadir of the right cusp are made. These are connected with an incision 1 cm below the valve, and a wedge of septal muscle is excised. |
Left Ventricular Tunnel Obstruction
When the left ventricular outflow tract is diffusely obstructed by a congenitally narrow tunnel, none of the aforementioned techniques is helpful to any significant degree. A left ventricular apical conduit to the ascending or descending aorta is an alternative, but not a favored one. The Rastan-Konno aortoventricular septoplasty, although a somewhat radical procedure, provides satisfactory results. In infants and children, a Ross-Konno procedure (replacing the aortic root with the pulmonary autograft, completing the ventriculoseptoplasty, and reconstructing the right ventricular outflow tract with a pulmonary homograft) is the operation of choice for this diagnosis.
Rastan-Konno Aortoventricular Septoplasty
Bicaval and aortic cannulations are made in the usual manner. On cardiopulmonary bypass with moderate cooling, the aorta is cross-clamped and cardioplegic arrest of the heart is achieved by the usual techniques (see Chapter 3). The aorta is incised anteriorly in a longitudinal direction. The incision is then extended downward under direct vision into the root of the aorta.
The direction of the aortotomy should be as far as possible to the left of the right coronary artery ostium, but not reaching the commissure between the right and left sinuses. This prevents injury to the ostium of the right coronary artery.
The anterior surface of the right ventricular outflow tract is then incised obliquely downward from the aortic root for a distance sufficient to provide good exposure of the interventricular septum (Fig. 24-5). Alternatively, the right ventriculotomy is made first and then extended upward into the aortic root.
The right ventricular outflow tract should be opened before cutting across the aortic annulus to ensure that the native pulmonic valve is not injured. Late pulmonary insufficiency is seen not infrequently following this procedure.
The possibility of abnormal distribution of right coronary artery branches crossing the right ventricular outflow tract to supply the left ventricular mass must be borne in mind when incising the infundibulum to prevent ischemic injury to the heart.
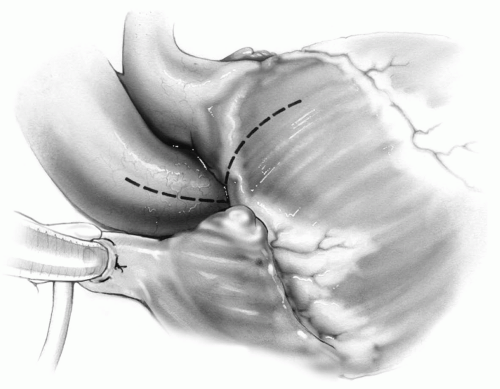 FIG 24-5. Oblique incision on the aortic root and incision on right ventricle to expose the interventricular septum in the Rastan-Konno aortoventricular septoplasty. |
The aortotomy is then continued obliquely downward across the aortic annulus onto the massively thickened interventricular septum (Fig. 24-6). The distorted aortic leaflets are then removed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


