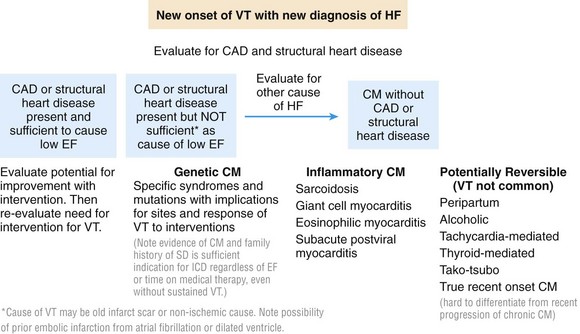
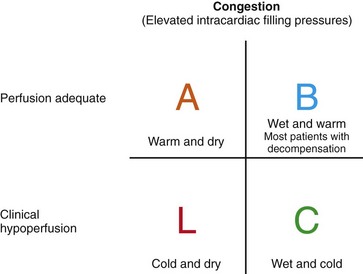
89 Ventricular arrhythmias may present simultaneously with the diagnosis of systolic dysfunction or heart failure. Rarely, incessant or very frequent ventricular tachycardia (VT) can actually cause heart failure. More commonly, VT or ventricular fibrillation (VF) arises in patients with known systolic dysfunction as a result of aggravating factors such as recurrent ischemia, drug effects, or electrolyte abnormalities, or as a herald of progression of underlying heart failure. Therapeutic options and prognosis for ventricular arrhythmias in the setting of heart failure are constrained by the cause and the clinical severity of the heart failure. In patients with mild to modest symptoms of heart failure (New York Heart Association [NYHA] Classes I and II), the annual risk of sudden death ranges between 2% and 6%, accounting for most of the mortality. With more advanced heart failure (NYHA Classes III and IV), the risk rises to 5% to 12% per year.1 Although the frequency of ventricular arrhythmias increases as heart failure worsens, unexpected sudden death accounts for less than half of mortality in advanced heart failure. Those with the worst heart disease gain the least in terms of survival after an aborted arrhythmic event caused by death from pump failure and other related comorbidities.2,3 Ventricular arrhythmia or sudden cardiac death may be the initial manifestation of cardiac disease.4 With clinical stabilization, the focus is on diagnosis of the underlying cause and any precipitating factors, with emphasis on treatable conditions. Implantable cardioverter-defibrillators (ICDs) generally are indicated for secondary prevention, except in the setting of specific reversible causes or anticipated early death from refractory hemodynamic decompensation or other terminal conditions. Potentially reversible causes to be identified and treated include left ventricular (LV) dysfunction related to stunning or hibernation from ischemia, some of the inflammatory myocardiitides, thyroid dysfunction, and alcoholic cardiomyopathy (Figure 89-1). Figure 89-1 Examples of causes of cardiomyopathy with particular relevance for those associated with ventricular arrhythmias. CAD, Coronary artery disease; CM, cardiomyopathy; EF, ejection fraction; HF, heart failure; VT, ventricular tachycardia. The electrocardiogram often provides the first clue to structural heart disease. Echocardiography is the first step taken to determine LV function, right ventricular (RV) function, and possible structural cardiac disease. Ventricular function is often worse after cardiac arrest or sustained VT, and reassessment after a period of recovery is typically necessary for a more accurate determination of the extent of underlying systolic impairment. In patients with low ejection fraction and extensive wall motion abnormalities, nuclear imaging may not be sensitive enough to exclude diffuse coronary artery disease. Hence, cardiac catheterization with coronary angiography should be performed to exclude or define coronary artery disease in patients for whom revascularization would be considered. Cardiac magnetic resonance (CMR) imaging is emerging as a valuable tool for detection of intramyocardial disease not readily evident on echocardiography, such as inflammation or focal scarring.5 Cardiac sarcoidosis is a particularly important cause of cardiomyopathy that is often undetected until presentation with ventricular arrhythmias or a new conduction block. Less than half of patients with evidence of cardiac sarcoid at autopsy will have had clinically apparent cardiac involvement. Patchy noncaseating granulomas tend to involve the basal ventricular septum with disruption of cardiac conduction. When the right ventricle is predominantly involved, a normal left ventricular ejection fraction (LVEF) may be falsely reassuring. Sudden cardiac death accounts for two-thirds of terminal events in patients with overt cardiac sarcoidosis.6,7 Early presentation with heart block should prompt a search for cardiac sarcoidosis in patients with systolic dysfunction. In a review of unexplained heart block in patients younger than 55 years of age, cardiac sarcoid or giant cell myocarditis accounted for 25% of cases, and these patients had a high incidence of sudden death or ventricular tachycardia or the need for cardiac transplantation.8 Although endomyocardial biopsy provides a definitive diagnosis, sensitivity is low at 10% to 20% because of the patchy nature of the disease distribution. CMR with gadolinium enhancement and positron emission tomography (PET) scanning are becoming valuable aids in diagnosis.6,7 Giant cell myocarditis is generally characterized by a more fulminant course with worse outcomes than sarcoidosis. The granulomas are accompanied by a diffuse inflammatory infiltrate. Although generally considered as distinct entities on the basis of biopsy and presentation, sarcoidosis and giant cell myocarditis may represent different levels along a spectrum of inflammation with giant cells. Hearts showing sarcoidosis on endomyocardial biopsy have occasionally been found to have areas consistent with giant cell myocarditis after removal at the time of transplantation. Cases of patients in whom giant cell myocarditis has been stabilized for a year or longer by high-dose immunosuppressive therapy have been reported.9,10 Postviral myocarditis is probably much more common than has been recognized. More than half of patients presenting within 3 months of subacute heart failure symptoms and low ejection fraction will show improvement in the LV ejection fraction to about 40% within the next 6 to 12 months.10 Endomyocardial biopsy performed in these patients often shows mild hypertrophy without evidence of cellular inflammation or significant fibrosis. Although premature ventricular contractions (PVCs) may occur, sustained VT or VF is uncommon in early stages of presumed postviral myocarditis. It should be noted that Lyme disease has been reported rarely to cause clinical myocarditis with or without clinical conduction system disease. Familial cardiomyopathies (CMs) account for 20% to 30% of cases of disease originally diagnosed as idiopathic dilated CM. Most cases are transmitted in an autosomal dominant pattern, but autosomal recessive, X-linked, and mitochondrial inheritance patterns are also well recognized. More than 30 genes have been identified as harboring mutations that cause familial dilated CM (DCM); however, mutations in these genes account for only half of the reported cases of familial DCM.11,12 Sarcomeric gene mutations account for one-third. Mutations in the gene coding for structural proteins of the nuclear lamina (lamin A and C) and in the SCN5A gene are particularly associated with conduction system disease and ventricular arrhythmias in association with DCM.12,13 Research findings suggest that abnormalities in the giant molecule titin may be among the most common causes of inherited CM frequently associated with ventricular arrhythmias.14 Arrhythmogenic RV cardiomyopathy (ARVC) due to defects in genes encoding for cardiac desmosomal proteins is predominantly an RV disease, but LV involvement is common and can precede RV manifestations.15 Approximately 50% of cases have a familial transmission with an autosomal dominant inheritance. Sudden death and ventricular arrhythmias are often the initial presentation frequently provoked by exercise. RV failure due to progressive myocardial loss is seen in later stages of the disease and may progress to a phase of biventricular failure that can mimic DCM. Autosomal recessive forms of ARVC due to defects in plakoglobin or desmoplakin result in cardiocutaneous syndromes that include Naxos disease and Carvajal syndrome.16 Prolonged periods of all forms of tachycardia, including frequent PVCs, are well recognized as a cause of reversible CM. Ventricular arrhythmia is uncommon in tachycardia-related CM unless it is the causative tachycardia. The diagnosis of tachycardia CM is often a retrospective one based on recovery of ventricular function after treatment of the arrhythmia. In one retrospective analysis of 174 patients with idiopathic PVCs referred for catheter ablation, LV dysfunction was present in 33%.17 The smallest PVC burden resulting in LV dysfunction was 10% over a 24-hour period, but a 24% PVC burden best differentiated the group that demonstrated CM from the group with preserved LV function. Data also suggest that the probability of LV dysfunction is related to QRS duration of the PVCs; frequent PVCs with a wider QRS (>150 milliseconds) are associated with greater risk of CM.18 Frequent runs of nonsustained VT, PVCs, or supraventricular arrhythmias should also be considered a potential cause of deteriorating LV function in cases of previously stable cardiomyopathy of another origin. The onset of ventricular arrhythmias in a previously stable heart failure patient may result from electrolyte abnormalities, ischemia, or intercurrent illness but often heralds the progression of underlying cardiac disease. Most clinically functional patients with LVEF <35% and long-standing heart failure symptoms will have an ICD in place. Analysis of the SCD-Heft trial data revealed that necessary ICD therapies were provided to 16% of patients over a mean follow-up of 45 months.19 The event rate is higher for patients who receive an ICD for secondary prevention.20 Several studies have shown an association of ICD shocks with reduced survival, with heart failure being an important cause of mortality.19,21 Ventricular arrhythmia in a patient with an ICD should prompt careful patient reassessment, even though the ICD may have promptly restored sinus rhythm. The original diagnosis may need to be reevaluated. In heart failure with known coronary artery disease, ischemia and infarction that contribute to hemodynamic deterioration and arrhythmias may occur without recognized angina. Baseline abnormalities of cardiomyopathy may mask typical diagnostic features; therefore perfusion stress imaging or coronary angiography is often required. In a significant proportion of patients after ICD shock, progressive ventricular remodeling is often evidenced by ventricular enlargement and declining LV ejection fraction.22 Development of bundle branch block by dys-synchronous contraction can further contribute to adverse ventricular remodeling. Identifying the type of ventricular arrhythmia is helpful in determining the cause. Monomorphic VT usually represents reentry involving regions of scar from prior infarction, inflammation, or surgery. A mix of fibrosis and surviving strands of myocardium allows for reentrant VTs that have a high recurrence rate—20% per year.23 Polymorphic VT is often associated with changing arrhythmia substrates. Migratory circuits around scars can lead to polymorphic VT, but acute myocardial ischemia and electrolyte disturbances should be major considerations because they are often easier to correct. Adverse effects of drugs that prolong the QT interval are more common in heart failure. Torsade de pointes VT typically induced by drugs such as sotalol and dofetilide often requires specific interventions such as discontinuation of the offending drug, intravenous administration of magnesium, correction of electrolyte derangements, and, occasionally, pacing at faster rates. Less frequently, implanted devices themselves may exert proarrhythmic effects. Pacing algorithms designed to minimize ventricular pacing are recognized to induce VT/VF through inadvertent induction of long-short intervals.24 Sinus tachycardia or supraventricular tachycardia detected in the VT zone of an ICD can trigger unnecessary antitachycardia pacing to induce VT or VF. The appearance of ventricular arrhythmia in close temporal proximity to the start of LV epicardial pacing should raise the possibility of related proarrhythmia.25 Inactivation of LV pacing may be necessary. If loss of cardiac resynchronization therapy (CRT) results in hemodynamic deterioration, cautious reinstitution of LV pacing after control of arrhythmia with drugs or ablation is attained is a possibility. Rarely, RV leads can trigger PVCs or sustained ventricular VT or VF. Repositioning of the lead has occasionally resulted in resolution of VT in such patients.26 Evaluation of heart failure disease severity is a major component of initial and serial management. Bedside assessment of baseline hemodynamic status allows broad triage into four hemodynamic profiles based on whether clinical evidence supports the presence of elevated filling pressures (wet or dry) and the adequacy or critical compromise of systemic perfusion (warm or cold) (Figure 89-2).27 In the setting of chronic heart failure, rales and peripheral edema are frequently absent despite severely elevated filling pressures, which should be suspected in patients with orthopnea or dyspnea on minimal exertion such as that associated with getting dressed. High pressures in chronic heart failure are best detected through experienced evaluation of jugular venous pressure and may also be identified from echocardiographic findings of dilated inferior vena cava and elevated pulmonary artery pressures. Hypoperfusion should be suspected in patients with a narrow pulse pressure, even if the systolic blood pressure is preserved, and in patients with vague mental status and cool calves and forearms. Many patients with hypoperfusion will have been intolerant of attempts to uptitrate ACEIs or β-blockers given to treat hypotension. Because functional capacity is not well correlated with the ejection fraction, careful questioning about daily activities and limiting symptoms is crucial for assessment of disease trajectory. Figure 89-2 Simple 2 × 2 table to indicate the general hemodynamic profiles of patients with low ejection fraction. Most are able to maintain good perfusion without evidence of elevated intracardiac filling pressures—“warm and dry.” Profile B is the most common profile of decompensation—“warm and wet”—which requires thorough diuresis. The patient presenting with profile C—“cold and wet”—usually requires major intervention before procedures can be performed safely and may in some cases require triage for assessment of potential candidacy for transplantation or mechanical circulatory support. Very few patients present with profile L—“cold and dry”—unless they have recently been treated aggressively. Such patients generally do not have resting symptoms but may have very limited cardiac reserve. (Adapted from Nohria A, Tsang SW, Fang JC, et al: Clinical assessment identifies hemodynamic profiles that predict outcomes in patients admitted with heart failure. J Am Coll Cardiol 41:1797-1804, 2003.) Baseline hemodynamic compromise requires aggressive correction, which, in most cases, should precede procedural interventions or initiation of neurohormonal antagonist therapies. β-Blocking agents and inhibitors of the renin-angiotensin system are remarkably beneficial over the long term but when given acutely can exacerbate hemodynamic compromise. When hemodynamic stabilization cannot be achieved, or when the hemodynamic profile remains uncertain, right-heart catheterization can be useful for clarifying right- and left-sided filling pressures, perfusion, and systemic and pulmonary vascular resistance to guide further therapy. Intravenous diuretic therapy is the mainstay of acute therapy for congestion. If inotropic therapy has been initiated to treat hypoperfusion and to improve diuretic response, neurohormonal antagonists should be initiated in small doses and escalated gradually. Careful uptitration over weeks to months is required to individualize “optimal” dosing, which frequently is lower than in trial populations, particularly for elderly patients.28 The role of the right ventricle in the progression of heart failure has been underrecognized and still remains difficult to track because of the difficulty associated with routine imaging of this chamber. Some causes of heart failure such as sarcoidosis and ARVC can affect the right ventricle early. The causes of heart failure in younger patients often affect both ventricles similarly from the onset. However, the main challenge to the right ventricle in chronic heart failure is usually presented by progressive left-sided congestion, as worsening mitral regurgitation and higher LV filling pressures contribute to secondary pulmonary hypertension and subsequent right-heart failure. RV dilatation and tricuspid regurgitation then contribute to renal dysfunction and further fluid retention. Chronic congestion of the liver and of the digestive system leads to malnutrition and increases inflammatory mediators in late-stage disease. In addition to indicating worse outcomes with heart failure, serious RV dysfunction identified on echocardiography increases risk and decreases “bail-out” options for procedures because it is a contraindication to long-term mechanical circulatory support.29
Ventricular Arrhythmias in Heart Failure
Evaluation of the Patient
Patients Presenting With Cardiac Arrest or Sustained Ventricular Tachycardia Without Prior Heart Failure Diagnosis
Inflammatory Myocarditis
Genetic Cardiomyopathy
Tachycardia-Related Cardiomyopathy
Evaluation of Ventricular Arrhythmias in Patients With Known Heart Failure
Triage and Management of Heart Failure
Assessment of Compensation
Titration of Neurohormonal Antagonists
Heart Failure Disease Progression
The Pivotal Right Ventricle
Ventricular Arrhythmias in Heart Failure



