Venting and Deairing of the Heart
Venting of the left side of the heart is an effective technique for cardiac decompression and air removal. It is particularly useful when a dry field is desired for precise repair of intracardiac defects.
Left Ventricular Apical Venting
The apex of the left ventricle provides a satisfactory and accessible site for venting and is particularly effective for removal of air trapped in the ventricular cavity. However, it is rarely used currently. Its relevance becomes important when left ventricular venting is necessary before repeat sternotomy (see Repeat Sternotomy section in Chapter 1).
Technique
The region of the left ventricular apex may be thin walled and covered by fat. The site chosen for insertion of the vent must be well away from the branches of the coronary arteries and free of loose myocardial fat. There can be bleeding from this ventricular site after removal of the vent catheter.
A double-armed, 2-0 nonabsorbable suture is passed in a U-shaped manner through a suitable site near the left ventricular apex buttressed with rectangular Teflon felt pledgets. The distance between the stitches on the Teflon felt should be equal to the diameter of the vent catheter. The suture ends are then passed through a narrow plastic tube as a tourniquet.
With a no. 15 knife blade, a 3- to 4-mm incision is made in the center of the U-shaped stitch. This opening in the left ventricular apex is then dilated with a hemostat so that the vent catheter can be introduced gently into the left ventricle. The tourniquet is then snugged down and secured to the vent catheter. If any catheter side hole remains outside the heart, the vent will be ineffective.
When the heart is beating, gravity siphonage of the vent is usually adequate to decompress the heart and/or remove trapped air bubbles. When the heart is fibrillating or motionless, particularly after the administration of cardioplegia, the vent should be connected to gentle suction with adequate negative pressure to decompress the heart. When the catheter is removed, the U-shaped stitch is tied down snugly and if necessary reinforced with a few simple sutures.
When an excessive length of the catheter is introduced into the left ventricle, its tip may cross the aortic valve and drain much of the pump flow. This problem can occur particularly in infants and small children (Fig. 4-1).
Excessive suction pressure can damage the left ventricular endocardium. For this reason, some vents have a double lumen and the second lumen can be left open to air. Alternatively, and probably a safer technique, the vent tubing can be vented with a one-way valve.
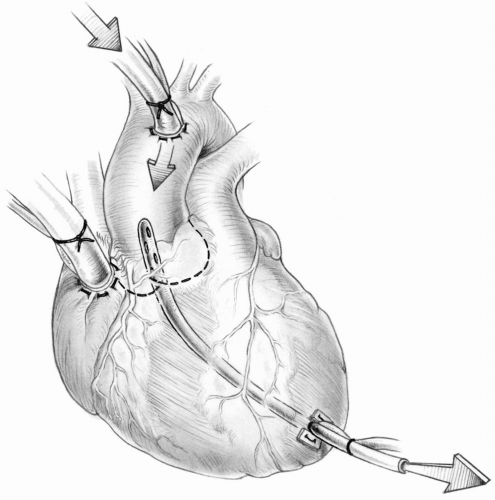  FIG 4-1. A vent catheter in the left ventricle crossing the aortic valve; pump flow is being suctioned. FIG 4-1. A vent catheter in the left ventricle crossing the aortic valve; pump flow is being suctioned. |
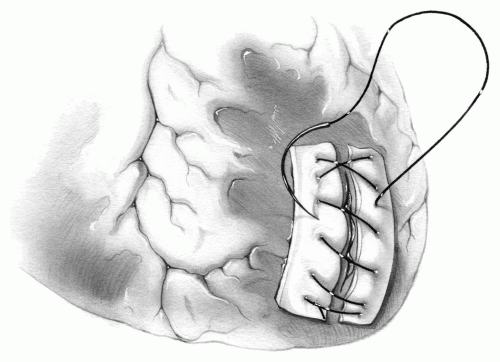 FIG 4-2. Repair of a tear in the left ventricular apex. |
When there is a tear or excessive bleeding from the left ventricular apex, the heart is decompressed. Long strips of Teflon felt with nonabsorbable sutures are used to repair the tear (Fig. 4-2). This is probably most safely accomplished with the heart arrested with cardioplegia.
If suction is too great or the apical opening is too large, air may be sucked into the left ventricular cavity around the vent site.
Venting through the Right Superior Pulmonary Vein
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


