Typical Carcinoid
Presentation
A 51-year-old woman is referred to your office for cough and hemoptysis. Upon questioning, she admits to having noted blood in the sputum for the past 6 months. She denies any weight loss but notes progressive weakness. The patient denies any history of smoking.
She had no other medical problems until 2 years ago when she was found to have asthma, recurrent bronchitis, and hypertension. Past medical history includes a cholecystectomy. Her medications include ipratropium bromide (Atrovent), enalapril maleate (Vasotec), and potassium supplements.
Vital signs include a systolic blood pressure of 140/90 mm Hg, normal sinus rhythm at 70 beats/min, and a respiratory rate of 20 breaths/min. On physical examination, you note wheezing on inspiration. The heart sounds are normal, and there are no murmurs. Abdominal examination demonstrates a soft, nontender, nondistended abdomen with a thick scar. The patient reports having had healing problems after undergoing a cholecystectomy.
Differential Diagnosis
The main causes of hemoptysis in a patient with a normal coagulation profile include inflammatory, pulmonary, and cardiac etiologies. Inflammatory causes include bronchitis, which is the most common cause of hemoptysis. Other causes include bronchiectasis, lung abscess, and infectious etiologies, such as tuberculosis and histoplasmosis. Pulmonary causes include primary lung cancer, bronchial neoplasms, lung contusion, and trauma by a foreign body. Finally, cardiac causes of hemoptysis include mitral stenosis and acute mitral regurgitation.
Discussion
In this patient, who is a nonsmoker, a primary lung cancer is less likely. However, the weakness, hypertension, hypokalemia, and physical examination findings are suggestive of a paraneoplastic syndrome. Given the recent diagnosis of asthma and bronchitis, the diagnosis of an endoluminal neoplasm should be strongly considered.
Recommendation
Laboratory evaluation of electrolytes and computed tomography (CT) scans of the chest.
Test Results
Sodium, 152; potassium, 3.2; chloride, 92; bicarbonate, 28. ▪
▪ CT Scans
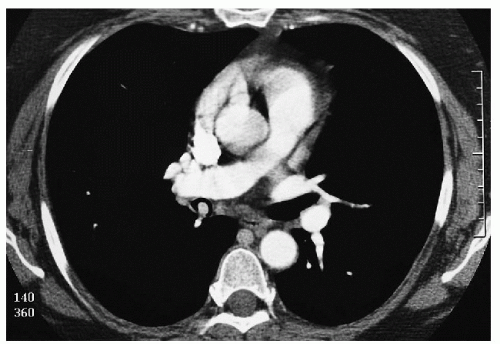 Figure 31-3 |
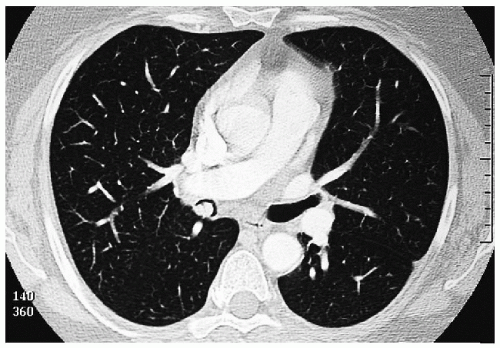 Figure 31-4 |
CT Scan Report
An endoluminal lesion with contrast enhancement is noted in the bronchus intermedius. There is no significant distal bronchiectasis or other postobstructive change. ▪
Discussion
The electrolyte levels are suggestive of hypercortisolism. The sources include pituitary or adrenal pathology as well as steroid secretion as part of a paraneoplastic syndrome. In this case, in which an abnormal mass is demonstrated on the CT scans, paraneoplastic syndrome is highly probable.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


