Esophageal Adenocarcinoma and Ivor Lewis Esophagectomy
Presentation
A 65-year-old man is referred to you for management of esophageal cancer after being diagnosed 3 months before his appointment. Initially, the patient reported a 2-month history of progressive dysphagia to solids and a 15-pound weight loss. Evaluation at that time consisted of computed tomography (CT) scan, barium swallow, and endoscopic ultrasound (EUS). Diagnostic evaluation and histologic biopsy demonstrated a lower esophageal adenocarcinoma with transmural penetration of the primary tumor, and there was no involvement of adjacent structures; however, one enlarged lymph node adjacent to the lesser gastric curvature was identified. The past medical history was unremarkable.
The patient underwent multimodality therapy including chemotherapy (two cycles of cisplatin and 5-fluorouracil) and external-beam radiotherapy (50 Gy), which was completed 2 weeks before his appointment. There was only a modest radiographic response to this therapy. In addition, the patient has persistent dysphagia to soft solids and has lost another 10 pounds.
▪ Chest X-ray
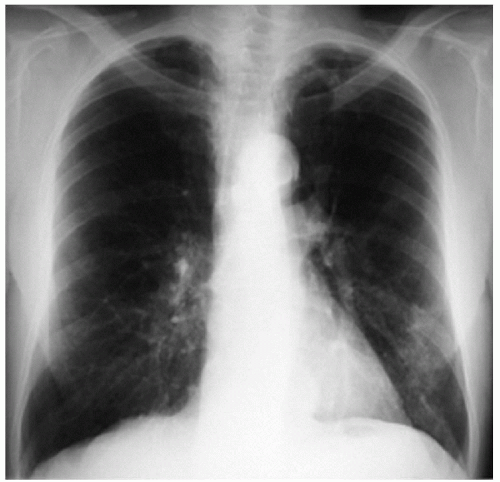 Figure 29-1 |
Chest X-ray Report
Findings consistent with diffuse emphysema. Mass effect in lower mediastinum adjacent to the left border of the spine. The heart is of normal size. There are no pleural effusions. ▪
▪ Barium Swallow
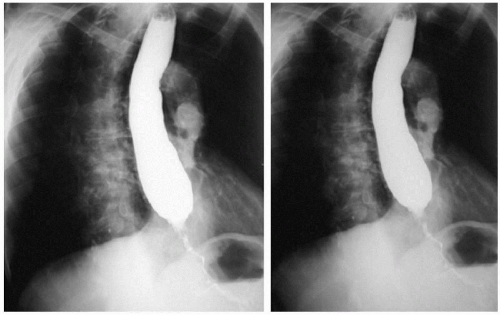 Figure 29-2 |
Barium Swallow Report
There is a mass in the lower thoracic esophagus with high-grade obstruction of the esophageal lumen. ▪
▪ CT Scan
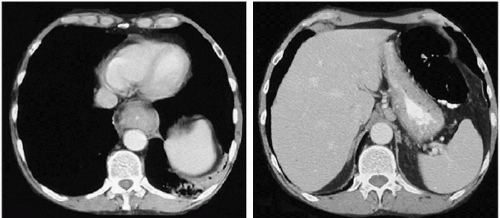 Figure 29-3 |
CT Scan Report
A mass is seen in the lower thoracic esophagus without obvious involvement of surrounding structures. Nonspecific infiltrate is seen at the base of the left lower lobe. An enlarged lymph node is seen adjacent to the lesser gastric curvature. Lungs are clear. Liver and adrenal glands are normal. ▪
Discussion
Despite the high frequency with which multimodality therapy for esophageal cancer is recommended, the benefit of multimodality treatment has not been proved. Most randomized studies demonstrate no apparent survival advantage for neoadjuvant chemotherapy, radiotherapy, or combined chemoradiotherapy. Studies suggest that there may be a survival advantage for neoadjuvant chemotherapy in patients with adenocarcinoma. Surgery remains an important component of potentially curative therapy for esophageal cancer.
Fortunately, there is no evidence that preoperative chemotherapy or radiation therapy has important adverse effects on intraoperative or postoperative complications. Neoadjuvant therapy does make the operation technically more difficult because normal tissue planes are sometimes obliterated after treatment. Transthoracic esophagectomy after radiation treatment allows dissection under direct vision, which is often a better technique than the so-called blind or blunt transhiatal esophagectomy technique.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


