Tuberculosis
Presentation
A 48-year-old man who has been living in homeless shelters for the past 3 years presents to the emergency department with a 1-week history of cough and hemoptysis. He was previously diagnosed with tuberculosis (TB) but has been noncompliant with multidrug therapy. Chest x-rays are performed on admission.
▪ Chest X-rays
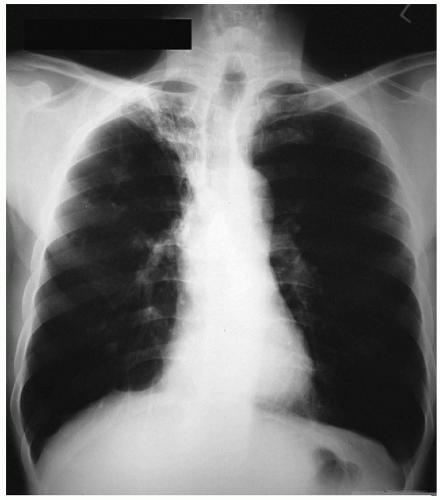 Figure 46-1 |
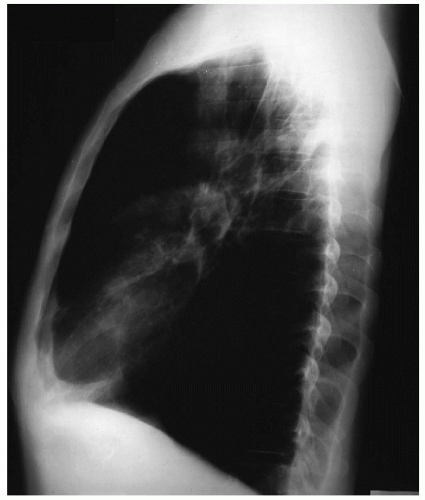 Figure 46-2 |
Chest X-ray Report
The chest x-rays demonstrate airspace disease in a collapsed right upper lobe with cephalad displacement of the major and minor fissures. There are no pleural effusions. The heart size is normal. ▪
Discussion
These findings are consistent with a chronic infectious process involving the right upper lobe and resulting in the destruction of lung parenchyma. This finding on the chest x-ray is most likely the result of untreated or inadequately treated TB in this middle-aged man who has lived an impoverished lifestyle. Hemoptysis might be due to TB infection, a coexisting bacterial infection, or bronchiectasis in the destroyed lung. A superinfection with fungus, such as Aspergillus species, might also account for the hemoptysis. An underlying malignancy should also be considered.
In the United States, the incidence of TB declined at a rate of 6% per year between 1953 and 1984, but since 1985, there has been an increase in the number of cases. This rise in incidence of TB has been attributed to the following factors: (a) the increased incidence of human immunodeficiency virus (HIV) infection, (b) immigration of people from areas of high prevalence of TB to the United States, and (c) social conditions such as homelessness and increased crowding in shelters, nursing homes, and prisons.
In the absence of massive hemoptysis (more than 600 mL within a 24-hour period), chest computed tomography (CT) scans with contrast infusion should be obtained for further evaluation.
▪ CT Scans
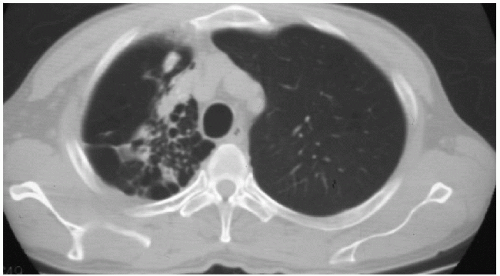 Figure 46-3 |
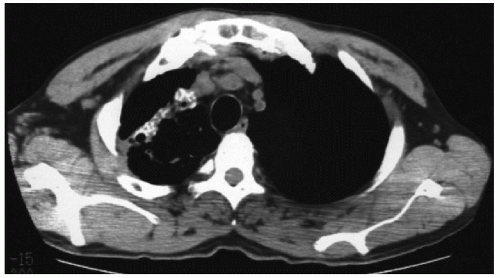 Figure 46-4 |
CT Scan Report
The chest CT confirms a largely destroyed right upper lobe with evidence of bronchiectasis. There are no enlarged mediastinal lymph nodes, and there is no evidence of pneumothorax or pleural effusions. ▪
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


