CHAPTER 104 Tumors of the Heart
Tumors of the heart are classified as either primary or secondary. Primary tumors arise in the heart and are either benign or malignant. Secondary tumors are metastases from primary tumors arising elsewhere and hence are always malignant. Primary tumors are rare, with an autopsy incidence of less than 0.1%.1 Secondary tumors are observed more commonly, with a postmortem incidence of about 1%.2 The prevalences of primary, benign neoplasms (Table 104-1); primary, malignant tumors (Table 104-2); and metastatic neoplasms (Table 104-3) were compiled by investigators at the Armed Forces Institute of Pathology.3,4
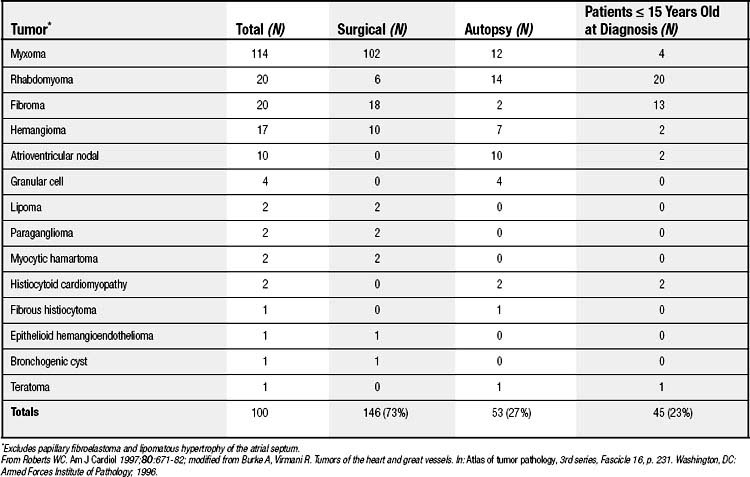
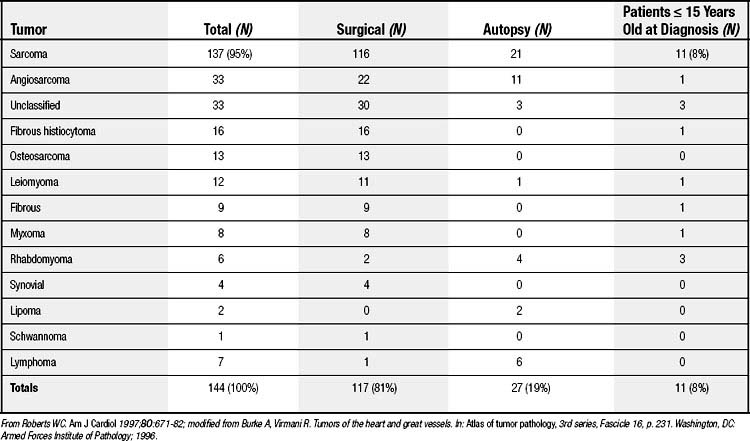
Table 104–3 Metastatic Neoplasms of the Heart at Necropsy∗
| Primary Tumor | Total Autopsies | Metastases to Heart |
|---|---|---|
| Lung | 1037 | 180 (17%) |
| Breast | 685 | 70 (10%) |
| Lymphoma | 392 | 67 (17%) |
| Leukemia | 202 | 66 (33%) |
| Esophagus | 294 | 37 (13%) |
| Uterus | 451 | 36 (8%) |
| Melanoma | 69 | 32 (46%) |
| Stomach | 603 | 28 (5%) |
| Sarcoma | 159 | 24 (15%) |
| Oral cavity and tongue | 235 | 22 (9%) |
| Colon and rectum | 440 | 22 (5%) |
| Kidney | 114 | 12 (11%) |
| Thyroid gland | 97 | 9 (9%) |
| Larynx | 100 | 9 (9%) |
| Germ cell | 21 | 8 (28%) |
| Urinary bladder | 128 | 8 (6%) |
| Liver and biliary tract | 325 | 7 (2%) |
| Prostate gland | 171 | 6 (4%) |
| Pancreas | 185 | 6 (3%) |
| Ovary | 188 | 2 (1%) |
| Nose (interior) | 32 | 1 (3%) |
| Pharynx | 67 | 1 (1%) |
| Miscellaneous | 245 | 0 |
| Total | 6240 | 653 (10%) |
∗ Listed in order of the number of metastases to the heart
From Roberts WC. Am J Cardiol 1997;80:671-82. Modified from Burke A, Virmani R (who combined studies of McAllister HA, Feoglio JJ Jr. Tumors of the cardiovascular system. In: Atlas of tumor pathology, 2nd series, Fascicle 15, p. 111. Washington, DC: Armed Forces Institute of Pathology; 1978; and Mukai K, Shinkai T, Tominaga K, Shimosato Y. The incidence of secondary tumors of the heart and pericardium: a 10-year study. Jpn J Clin Oncol 1988;18:195).
Cardiac tumors present with variable clinical features. Symptoms are frequently determined by the intracardiac location of the tumor. Intracavitary tumors can obstruct blood flow, causing signs and symptoms that mimic those of valvular heart disease. Intracavitary tumors can also cause embolic events, resulting in symptoms related to the site of embolization. Intramyocardial tumors can trigger cardiac rhythm disturbances, including sudden death.5 Cardiac tumors can also cause systemic symptoms mimicking collagen vascular disease, malignancy, or infective endocarditis.5
BENIGN PRIMARY CARDIAC TUMORS
Myxomas
Definition, Incidence, and Prevalence
Myxomas are the most common primary cardiac tumors. They are benign. Although they have been reported in both sexes and in all age groups, they most often occur in women in the third to sixth decade of life. Myxomas are usually sporadic, but at least 7% occur as part of an autosomal dominant syndrome. In the latter situation, the myxoma is a component of a larger syndrome referred to as the Carney complex.6 In the Carney complex, myxomas are associated with spotty pigmentation of the skin and endocrine hyperactivity. Myxomas that arise as part of the Carney complex affect both sexes equally and at any age, arise as single or multiple lesions in all chambers of the heart, and tend to recur after surgical excision.7
Morphology
Arising from the endocardium, myxomas usually extend into a cardiac chamber. They are generally polypoid, pedunculated lesions with a smooth surface that may be covered with thrombus (Fig. 104-1). The tumors range in size from 1 to 15 cm, but they are most commonly about 5 cm in diameter with a weight of approximately 70 g.8–11 Myxomas are thought to arise from pluripotent mesenchymal cells. Histologically, they consist of a matrix of acid mucopolysaccharide (Fig. 104-2).12 The cells are polygonal or spindle-shaped and may form capillary-like channels that can communicate with arteries and veins located at the base of the tumor.10
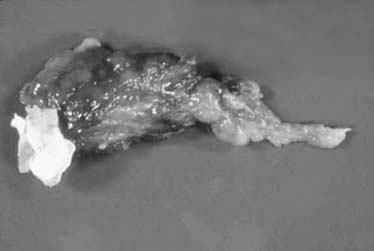
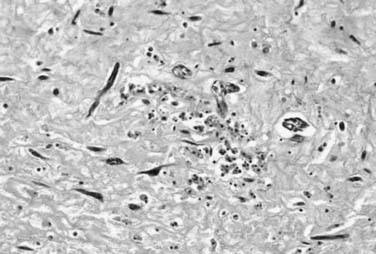
Figure 104–2 Hematoxylin and eosin stain of myxoma. (See color version in the online edition through Expert Consult.)
Myxomas most commonly occur in the atria. Approximately 75% arise in the left atrium, and 15% to 20% arise in the right atrium.10 Most left atrial myxomas are located on the border of the fossa ovalis, but they can originate from any place on the atrial wall. The remainder of myxomas are located in the ventricles. Myxomas arising from cardiac valves are rare.
Clinical Characteristics
Because most myxomas arise in the left atrium, systemic embolization is common, occurring in 30% to 50% of cases.13–15 Left ventricular myxomas have an even higher propensity to embolize.16 Right atrial myxomas rarely display clinical manifestations of emboli. Embolic material from myxomas can compromise blood flow to any organ, but the brain is most commonly affected. Myxoma should be included in the differential diagnosis of any systemic embolic event, and any embolic material removed should undergo histologic evaluation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


