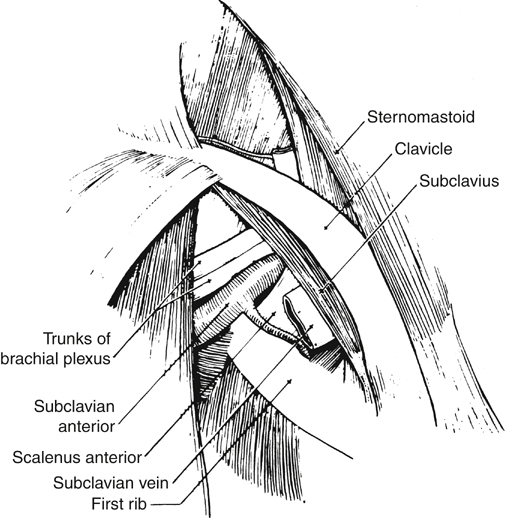
The thoracic outlet syndrome (TOS) encompasses a variety of conditions caused by compression of the neurovascular structures passing between the clavicle, the scalene muscles, and the first rib (Figure 1). When a patient’s symptoms warrant operative therapy, transaxillary first rib resection can be performed successfully in most cases. Varying therapeutic approaches for the different manifestations of TOS exist (Table 1). TABLE 1 Therapeutic Preferences for the Different Components of Thoracic Outlet Syndrome Proper patient selection is an important determinant of results after transaxillary rib resection for neurologic symptoms (Table 2). The decision to operate should be made only after a complete neurologic evaluation has excluded any other entity that could cause similar symptoms. TABLE 2 Indications for Operation in Neurologic Thoracic Outlet Syndrome
Transaxillary Operative Management of Thoracic Outlet Syndrome
Syndrome
Preferred Approach
Comments
Venous compression
Transaxillary first rib resection
Timing contested (immediate vs. 6-week wait), but consensus for immediate surgery is emerging
Venous with thrombosis (chronic)
Transaxillary first rib resection
Relieves compression of collateral veins; if venous reconstruction is required, the best approach is anterior
Arterial with cervical rib
Supraclavicular
Cervical ribs associated with arterial pathology are usually very wide and difficult to remove from the axilla
Arterial with aneurysm
Supraclavicular and infraclavicular
Cosmetically better than claviculectomy, which gives the same exposure
Arterial without bony or vascular pathology
Transaxillary first rib resection
Unusual presentation, old anterior scalene syndrome?
Neurologic
Transaxillary first rib resection
Best decompression with lowest incidence of recurrence (R. Saunders)
Neurologic with cervical rib
Transaxillary first rib resection
Ribs are usually very narrow and can be removed through the axilla along with the first rib
Operation
Condition
Comments
Transaxillary rib resection with division of fibrous band from C7
Atrophy of the ulnar innervated muscles
Classic TOS; very rare, but no one would debate its existence or indication for operation; atrophy persists after operation
Avoid operation (poor results, especially in women)
Repetitive work-related injury
Makes up part of the “disputed” neurologic TOS; many doubt the existence of this entity
Transaxillary rib resection
Symptoms reproduced by abduction of the shoulder
Patients must be screened carefully but good results can be achieved
Supraclavicular large rib resection, Transaxillary small rib resection
Symptoms in the presence of a cervical rib
Presence of a cervical rib makes the diagnosis of TOS more certain
Any operation results in poor outcome
Symptoms with chronic denervation on electrodiagnostic studies
TOS rarely causes permanent nerve damage
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


