Thymoma
Presentation
A 52-year-old woman with no significant past medical history presents to your office after she was seen by her primary medical doctor with symptoms of ptosis and diplopia. She is a nonsmoker. On examination, there are decreased breath sounds over the left lung field. The patient presents with the following chest x-rays.
▪ Chest X-rays
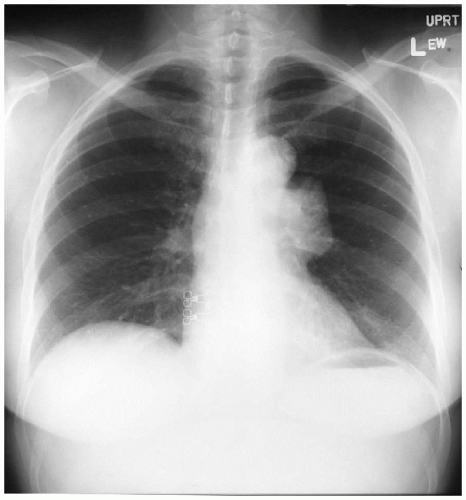 Figure 50-1 |
 Figure 50-2 |
Chest X-ray Report
Lung fields are clear; the heart is of normal size. Both diaphragms are visualized. A round anterior mediastinal mass is present. ▪
Differential Diagnosis
The differential diagnosis for anterior mediastinal masses in the adult includes thymoma, lymphoma, thyroid, and germ cell tumor. In children, the differential diagnosis for mediastinal masses includes germ cell tumors and lymphoma. In this patient with symptoms of ptosis, diplopia, and an anterior mediastinal mass, one must consider myasthenia gravis to be the primary diagnosis.
Discussion
Fifteen percent of patients with myasthenia gravis have a thymoma. In contrast, 30% to 50% of patients with thymoma have myasthenia gravis. The incidence of thymoma is equal in male and female patients. This is in contrast to myasthenia gravis, in which the female-to-male ratio is 2:1. Symptoms may include ptosis, ophthalmoplegia, dysarthria, and dysphagia. Severity of weakness increases during the day, especially after use of affected muscle groups. The syndrome is characterized by autoantibodies to acetylcholine (ACH) receptors. In addition, the ACH receptor concentration at the neuromuscular end plate is reduced.
The initial diagnostic test is the Tensilon test (edrophonium chloride), which is a short-acting anticholinesterase. Response to the Tensilon test is within 45 to 60 seconds; patients may also experience salivation, sweating, and nausea. Blood tests for antibodies against ACH receptors are elevated in most patients. Normal levels of ACH receptor antibody do not exclude the diagnosis of myasthenia gravis. Other tests may include repetitive nerve stimulation and single-fiber electromyography.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


