CHAPTER 26 Thoracic Outlet Syndrome and Dorsal Sympathectomy
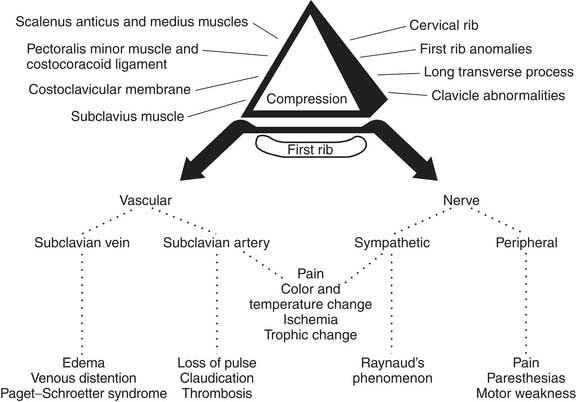
Thoracic outlet syndrome, a term coined by Rob and Standover,1 refers to compression of the subclavian vessels and brachial plexus at the superior aperture of the chest. It was previously designated, according to presumed etiologies, as scalenus anticus, costoclavicular, hyperabduction, cervical rib, and first thoracic rib syndromes. The various syndromes are similar, and the compression mechanism is often difficult to identify. Most compressive factors operate against the first rib (Fig. 26-1).2,3
HISTORICAL ASPECTS
Until 1927, the cervical rib was commonly thought to be the cause of symptoms of this syndrome. Galen and Vesalius first described the presence of a cervical rib.4 Hunauld, who published an article in 1742, is credited by Keen5 as being the first to describe the importance of the cervical rib in causing symptoms. In 1818, Cooper treated symptoms of cervical rib with some success,6 and in 1861, Coote7 did the first cervical rib removal. Halsted8 stimulated interest in dilation of the subclavian artery distal to cervical ribs, and Law9 reported the role of adventitious ligaments in the cervical rib syndrome. In 1927, Adson and Coffey6 suggested the role of the scalenus anticus muscle in cervical rib syndrome. Naffziger and Grant10 and Ochsner and associates11 popularized sectioning of the scalenus anticus muscle. Falconer and Weddell12 and Brintnall and colleagues13 incriminated the costoclavicular membrane in the production of neurovascular compression. In 1945, Wright14 described the hyperabduction syndrome with compression in the costoclavicular area by the tendon of the pectoralis minor. Rosati and Lord15 added claviculectomy to anterior exploration, scalenotomy, cervical rib resection (when one was present), and sectioning of the pectoralis minor and subclavian muscles and of the costoclavicular membrane. The role of the first rib in causing symptoms of neurovascular compression was recognized by Bramwell16 in 1903. Murphy17 is credited with the first resection of the first rib. Brickner,18 Brickner and Milch,19 and Telford and coworkers20,21 suggested that the first rib was the culprit. Clagett2 emphasized the first rib and its resection through the posterior thoracoplasty approach to relieve neurovascular compression. In 1962, Falconer and Li22 reported the anterior approach for first rib resection, whereas Roos23 introduced the transaxillary route for first rib resection and extirpation. Caldwell and colleagues24 introduced the method of measuring motor conduction velocities across the thoracic outlet in diagnosing thoracic outlet syndrome. Urschel and Razzuk25 popularized reoperation for recurrent thoracic outlet syndrome.
SURGICAL ANATOMY
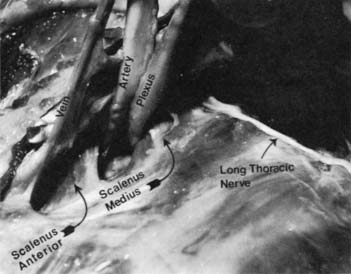
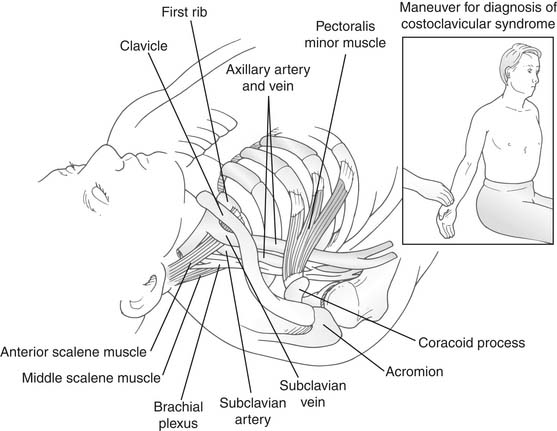
At the superior aperture of the thorax, the subclavian vessels and the brachial plexus traverse the cervicoaxillary canal to reach the upper extremity. The cervicoaxillary canal is divided by the first rib into two sections: the proximal one, composed of the scalene triangle and the costoclavicular space, and the distal one, composed of the axilla. The proximal division is the more critical for neurovascular compression. It is bounded superiorly by the clavicle, inferiorly by the first rib, anteromedially by the costoclavicular ligament, and posterolaterally by the scalenus medius muscle and the long thoracic nerve. The scalenus anticus muscle, which inserts on the scalene tubercle of the first rib, divides the costoclavicular space into two compartments: the anteromedial one containing the subclavian vein and the posterolateral one containing the subclavian artery and the brachial plexus (Fig. 26-2). The latter compartment, which is bounded by the scalenus anticus anteriorly, the scalenus medius posteriorly, and the first rib inferiorly, is called the scalene triangle.
FUNCTIONAL ANATOMY
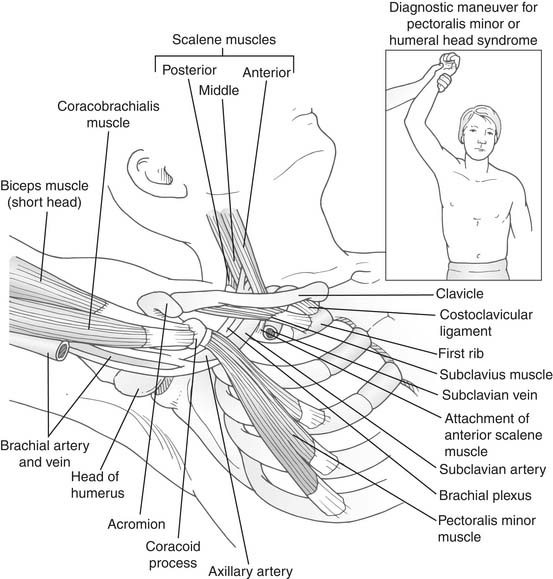
The cervicoaxillary canal, particularly its proximal segment, the costoclavicular area, normally has ample space for passage of the neurovascular bundle without compression. Narrowing of this space occurs during functional maneuvers. It narrows during abduction of the arm because the clavicle rotates backward toward the first rib and the insertion of the scalenus anticus muscle. In hyperabduction, the neurovascular bundle is pulled around the pectoralis minor tendon, the coracoid process, and the head of the humerus. During this maneuver, the coracoid process tilts downward and thus exaggerates the tension on the bundle. The sternoclavicular joint, which ordinarily forms an angle of 15 to 20 degrees, forms a smaller angle when the outer end of the clavicle descends (as in drooping of the shoulders in poor posture), and narrowing of the costoclavicular space may occur.15 Normally, during inspiration, the scalenus anticus muscle raises the first rib and thus narrows the costoclavicular space. This muscle may cause an abnormal lift of the first rib, as in cases of severe emphysema or excessive muscular development, which is seen in young adults.
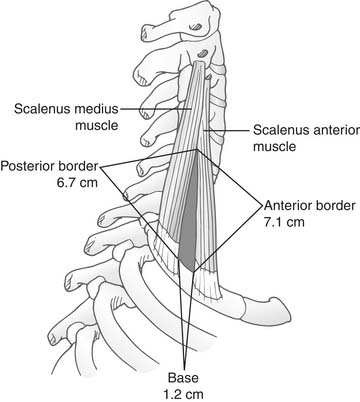
The scalene triangle, which normally occurs between the scalenus anticus anteriorly, the scalenus medius posteriorly, and the first rib inferiorly, permits the passage of the subclavian artery and the brachial plexus, which are in direct contact with the first rib. The space of the triangle is 1.2 cm at its base and approximately 6.7 cm in height (Fig. 26-3). There is a close-fitting relationship between the neurovascular bundle and this triangular space. Anatomic variations may narrow the superior angle of the triangle, cause impingement on the upper components of the brachial plexus, and produce the upper type of scalenus anticus syndrome that involves the trunk containing elements of C5 and C6. If the base of the triangle is raised, compression of the subclavian artery and the trunk containing components of C7, C8, and T1 results in the lower type of scalenus anticus syndrome. Both types have been described by Swank and Simeone.26
COMPRESSION FACTORS
Many factors may cause compression of the neurovascular bundle at the thoracic outlet, but the basic factor is deranged anatomy, to which congenital, traumatic, and, occasionally, atherosclerotic factors may contribute (Box 26-1).15 Bony abnormalities are present in approximately 30% of patients, either as cervical rib, bifid first rib, and fusion of first and second ribs; clavicular deformities; or previous thoracoplasties.3 These abnormalities can be visualized on the plain posteroanterior chest film, but special radiographic views of the lower cervical spine may be required in some cases of cervical ribs.
SYMPTOMS AND SIGNS
The symptoms of thoracic outlet syndrome depend on whether the nerves or blood vessels, or both, are compressed in the cervicoaxillary canal. Neurogenic manifestations are observed more frequently than vascular ones. Symptoms consist of pain and paresthesias, which are present in approximately 95% of cases, and motor weakness and occasionally atrophy of hypothenar and interosseous muscles, which is the ulnar type of atrophy, in approximately 10%. The symptoms occur most commonly in areas supplied by the ulnar nerve, which include the medial aspects of the arm and hand, the fifth finger, and the lateral aspects of the fourth finger. The onset of pain is usually insidious and commonly involves the neck, shoulder, arm, and hand. The pain and paresthesias may be precipitated by strenuous physical exercise or sustained physical effort with the arm in abduction and the neck in hyperextension. Symptoms may be initiated by sleeping with the arms abducted and the hands clasped behind the neck. In other cases, trauma to the upper extremities or the cervical spine is a precipitating factor. Physical examination may be noncontributory. When present, objective physical findings usually consist of hypesthesia along the medial aspects of the forearm and hand. Atrophy, when evident, is usually described in the hypothenar and interosseous muscles with clawing of the fourth and fifth fingers. In the upper type of thoracic outlet syndrome, in which components of C5 and C6 are involved in compression, pain is usually in the deltoid area and the lateral aspects of the arm. The presence of this pain should induce action to exclude a herniated cervical disc.15 Entrapment of C7 and C8 components that contribute to the median nerve produces symptoms in the index finger and sometimes the middle finger. Components of C5, C6, C7, C8, and T1 can occur at the thoracic outlet by a cervical rib and produce symptoms of various degrees in the distribution of these nerves (Fig. 26-4).
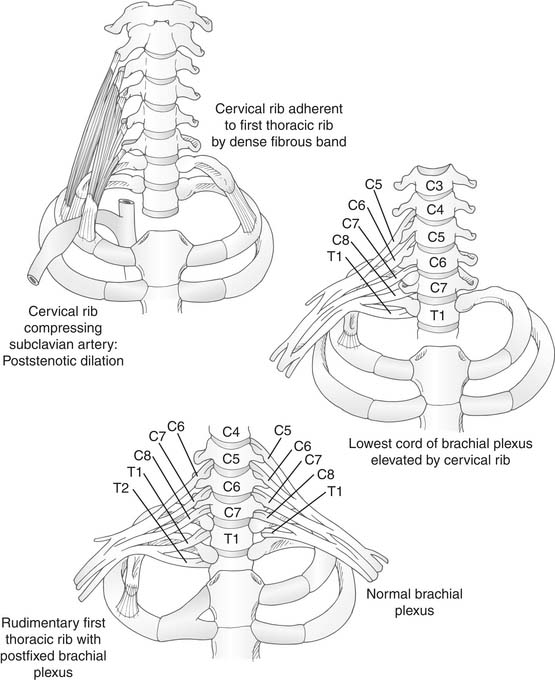
Figure 26–4 Compression caused by congenital rib abnormalities.
(Reprinted from www.netterimages.com @ elsevier Inc. All rights reserved.)
In some patients, the pain is atypical, involving the anterior chest wall or parascapular area, and is termed pseudoangina because it simulates angina pectoris. These patients may have normal coronary arteriograms and ulnar nerve conduction velocities decreased to values of 48 m/sec and less, which strongly suggests the diagnosis of thoracic outlet syndrome. The shoulder, arm, and hand symptoms that usually provide the clue for the diagnosis of thoracic outlet syndrome may initially be absent or minimal compared with the severity of the chest pain. The diagnosis of thoracic outlet syndrome is frequently overlooked; many of these patients are committed to becoming “cardiac cripples” without an appropriate diagnosis, or they develop severe psychological depression when told that their coronary arteries are normal and that they have no significant cause for their pain.27
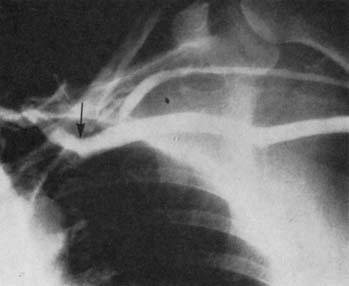
Symptoms of arterial compression include coldness, weakness, easy fatigability of the arm and hand, and pain that is usually diffuse.28,29 Raynaud’s phenomenon is noted in approximately 7.5% of patients with thoracic outlet syndrome.28 Unlike Raynaud’s disease, which is usually bilateral and symmetrical and elicited by cold or emotion, Raynaud’s phenomenon in neurovascular compression is usually unilateral and is more likely to be precipitated by hyperabduction of the involved arm, turning of the head, or carrying of heavy objects. Sensitivity to cold may also be present. Symptoms include sudden onset of cold and blanching of one or more fingers, followed slowly by cyanosis and persistent rubor. Vascular symptoms in neurovascular compression may be precursors of permanent arterial thrombosis.15 Arterial occlusion, usually of the subclavian artery, when present, is manifested by persistent coldness, cyanosis or pallor of the fingers, and in some instances, ulceration or gangrene. Palpation in the parascapular area may reveal prominent pulsation, which indicates poststenotic dilation or aneurysm of the subclavian artery (Fig. 26-5).30

Less frequently, the symptoms are those of venous obstruction or occlusion, commonly recognized as effort thrombosis, or Paget-Schroetter syndrome. The condition characteristically results in edema, discoloration of the arm, distention of the superficial veins of the limb and shoulder, and some degree of aches and pains. In some patients, the condition is observed on waking; in others, it follows sustained efforts with the arm in abduction. Sudden backward and downward bracing of the shoulders or heavy lifting or strenuous physical activity involving the arm may constrict the vein and initiate venospasm, with or without subsequent thrombosis. On examination, in cases of definite venous thrombosis, there is usually moderate tenderness over the axillary vein, and a cordlike structure may be felt that corresponds to the course of the vein. The acute symptoms may subside in a few weeks or days as the collateral circulation develops. Recurrence follows with inadequacy of the collateral circulation.31
Objective physical findings are more common in patients with primarily vascular rather than neural compression. Loss or diminution of radial pulse and reproduction of symptoms can be elicited by the three classic clinical maneuvers: the Adson’s or scalene test,32 the costoclavicular test, and the hyperabduction test.33
DIAGNOSIS
The diagnosis of thoracic outlet syndrome includes history, physical and neurologic examinations, films of the chest and cervical spine, electromyogram, and ulnar nerve conduction velocity (UNCV). In some cases with atypical manifestations, other diagnostic procedures such as cervical myelography, peripheral30 or coronary arteriography, or phlebography34 should be considered. A detailed history and physical and neurologic examinations can often result in a tentative diagnosis of neurovascular compression. This diagnosis is strengthened when one or more of the classic clinical maneuvers is positive and is confirmed by the finding of decreased UNCV.35
Clinical Maneuvers
The clinical evaluation is best based on the physical findings of loss or decrease of radial pulses and reproduction of symptoms that can be elicited by the following three classic maneuvers15,33:
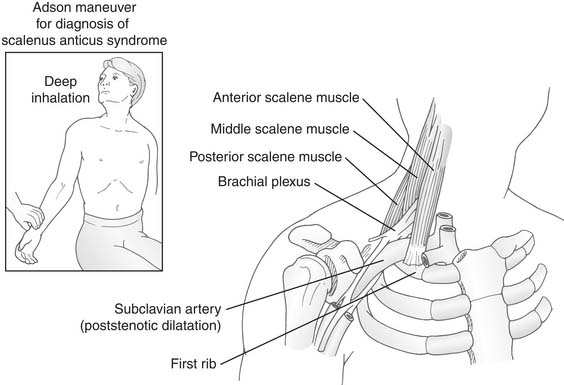
Figure 26–6 Adson’s maneuver. Relationship of the scalene triangle to the neurovascular bundle.
(Reprinted from www.netterimages.com @ elsevier inc. All rights reserved.)
Radiographic Findings
Films of the chest and cervical spine are helpful in revealing bony abnormalities, particularly cervical ribs (Fig. 26-9) and bony degenerative changes. If osteophytic changes and intervertebral space narrowing are present on plain cervical films, a cervical computed tomography (CT) scan should be obtained to rule out bony encroachment and narrowing of the spinal canal and the intervertebral foramina.

Nerve Conduction Velocity and Electromyography
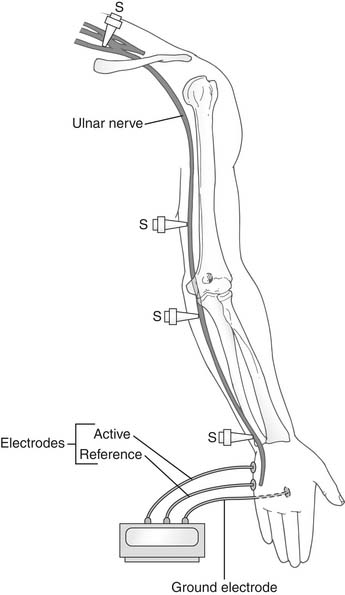
This test is widely used in differential diagnosis of the causes of arm pain, tingling, and numbness with or without motor weakness of the hand. Such symptoms may result from compression at various sites: in the spine; at the thoracic outlet; around the elbow, where it causes tardy ulnar nerve palsy; or on the flexor aspects of the wrist, where it produces carpal tunnel syndrome. For diagnosis and localization of the site of compression, cathodal stimulation is applied at various points along the course of the nerve. Motor conduction velocities of the ulnar, median, radial, and musculocutaneous nerves can be measured reliably.36 Caldwell and colleagues24 have improved the technique of measuring UNCV for evaluation of patients with thoracic outlet compression. Conduction velocities over proximal and distal segments of the ulnar nerve are determined by recording the action potentials generated in the hypothenar or first dorsal interosseous muscles. The points of stimulation are the supraclavicular fossa, middle upper arm, below the elbow, and at the wrist (Fig. 26-10).29
Method of Measuring Conduction Velocities
Equipment
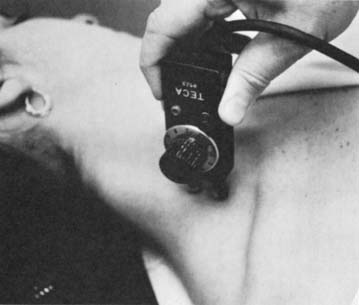
Electromyographic examination of each upper extremity and determination of the conduction velocities are done with the Meditron 201 AD or 312 or the TECA-3 electromyograph; coaxial cable with three needles or surface electrodes are used to record muscle potentials, which appear on the fluorescent screen (Fig. 26-11).

Technique
The conduction velocity is determined by the Krusen-Caldwell technique.24 The patient is placed on the examination table with the arm fully extended at the elbow and in about 20 degrees of abduction at the shoulder to facilitate stimulation over the course of the ulnar nerve. The ulnar nerve is stimulated at the four points by a special stimulation unit (Fig. 26-12) that imparts an electrical stimulus with strength of 350 V with the patient’s load, which is approximately equal to 300 V with the patient’s load with a skin resistance of 5000 Ω. Supramaximal stimulation is used at all points to obtain maximal response. The duration of the stimulation is 0.2 msec, except for muscular individuals, for whom it is 0.5 msec. Time of stimulation, conduction delay, and muscle response appear on the TECA screen; time markers occur each millisecond on the sweep.
Calculation of Velocities
After the latencies, which are expressed in milliseconds, are obtained, the distance in millimeters between two adjacent sites of stimulation is measured with steel tape. The velocities, which are expressed in meters per second, are calculated by subtracting the distal latency from the proximal latency and dividing the distance between two points of stimulation by the latency difference (Fig. 26-13) according to the following formula:
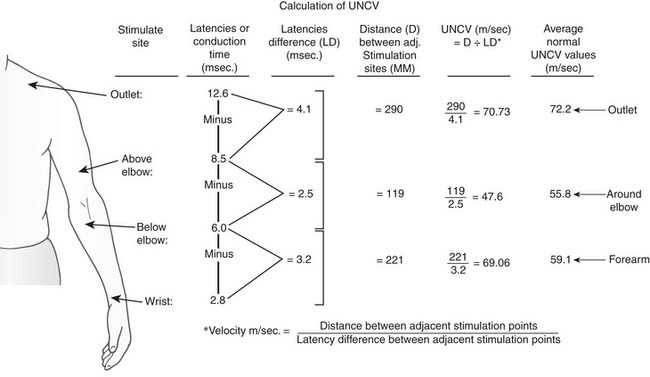
Figure 26–13 The sites of stimulation and the formula for calculating ulnar nerve conduction velocity (UNCV).

Normal Ulnar Nerve Conduction Velocities
The normal values of the UNCVs according to the Krusen-Caldwell technique24 are 72 m/sec or greater across the outlet, 55 m/sec or greater around the elbow, and 59 m/sec or greater in the forearm. Wrist delay is 2.5 to 3.5 msec. Decreased velocity in a segment or increased delay at the wrist indicates compression, injury, neuropathy, or neurologic disorders. Decreased velocity across the outlet is consistent with thoracic outlet syndrome. Decreased velocity around the elbow signifies ulnar nerve entrapment or neuropathy. Increased delay at the wrist is encountered in carpal tunnel syndrome.
Angiography
Simple clinical observations usually suffice to determine the degree of vascular impairment in the upper extremity. Peripheral angiography30,37 is indicated in some cases, as in the presence of a paraclavicular pulsating mass, the absence of radial pulse, or the presence of supraclavicular or infraclavicular bruits. Retrograde or antegrade arteriograms of the subclavian and brachial arteries to demonstrate or localize the pathology should be obtained. In cases of venous stenosis or obstruction, as in Paget-Schroetter syndrome, phlebograms are used to determine the extent of thrombosis and the status of the collateral circulation (Fig. 26-14).
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


