Figure 24.1 The thoracic duct usually lies in the posterior mediastinum, between the azygous vein, aorta, and esophagus.
 PREOPERATIVE PLANNING
PREOPERATIVE PLANNING
 Lymphangiography is a difficult study to perform and its application is limited by local expertise. However, if available, this study can be a useful adjunct to preoperative planning. Lymphangiography can clarify the anatomy of the thoracic duct and potentially identify duplicate or aberrant anatomy. The study may also identify the leak (Fig. 24.2). If the expertise is available, an attempt at embolization of the thoracic duct is reasonable. Lymphangiography is most useful in complicated chyle leaks where the etiology or source of the leak is unclear or in situations where mass ligation fails to control the leak.
Lymphangiography is a difficult study to perform and its application is limited by local expertise. However, if available, this study can be a useful adjunct to preoperative planning. Lymphangiography can clarify the anatomy of the thoracic duct and potentially identify duplicate or aberrant anatomy. The study may also identify the leak (Fig. 24.2). If the expertise is available, an attempt at embolization of the thoracic duct is reasonable. Lymphangiography is most useful in complicated chyle leaks where the etiology or source of the leak is unclear or in situations where mass ligation fails to control the leak.
 Enteral administration of cream may aid in visualization of the chyle leak. Cream should be given 30 to 60 minutes before operation to enhance the flow of chyle during inspection of the chest. This can be administered through a nasogastric or orogastric tube after induction of anesthesia.
Enteral administration of cream may aid in visualization of the chyle leak. Cream should be given 30 to 60 minutes before operation to enhance the flow of chyle during inspection of the chest. This can be administered through a nasogastric or orogastric tube after induction of anesthesia.
 The surgeon should ensure adequate volume resuscitation preoperatively.
The surgeon should ensure adequate volume resuscitation preoperatively.
 An epidural catheter should be placed if the initial catheter has been removed.
An epidural catheter should be placed if the initial catheter has been removed.
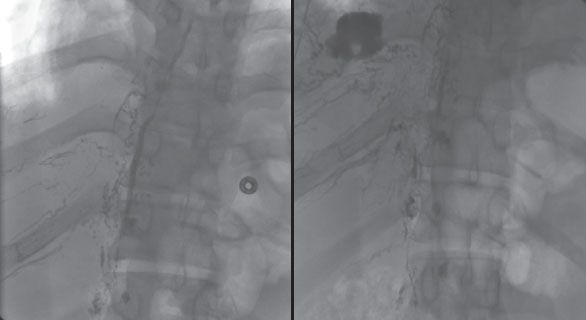
Figure 24.2 Lymphangiography can demonstrate the anatomy of the thoracic duct as well as the location of a thoracic duct injury. This lymphangiogram demonstrates the main thoracic duct in its normal anatomical location and a chyle leak into the right pleural space.
 The drainage tube for the gastric conduit (retrograde gastrostomy or nasogastric tube) should remain to intermittent suction to drain the conduit and reduce the risk of aspiration with induction of anesthesia.
The drainage tube for the gastric conduit (retrograde gastrostomy or nasogastric tube) should remain to intermittent suction to drain the conduit and reduce the risk of aspiration with induction of anesthesia.
 A double-lumen endotracheal tube is mandatory for visualization.
A double-lumen endotracheal tube is mandatory for visualization.
 Preoperative planning is similar for open or thoracoscopic visualization of the thoracic duct.
Preoperative planning is similar for open or thoracoscopic visualization of the thoracic duct.
 SURGERY
SURGERY
The technique of thoracic duct ligation is discussed for two scenarios: Ligation following transthoracic esophagectomy and VATS thoracic duct ligation for spontaneous chylothorax. The approaches and technical steps discussed apply to most indications for duct ligation.
Thoracic Duct Ligation Following Transthoracic Esophagectomy
Positioning
The patient is positioned in the left lateral decubitus position, rotated slightly forward. This positioning is identical to that used for Ivor Lewis esophagectomy. If the esophagectomy was performed in a minimally invasive fashion, the patient should be positioned as for that procedure.
Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


