CHAPTER 42 The Middle Mediastinum
DIAGNOSTIC MODALITIES
Imaging
The chest radiograph often provides the first glimpse of a possible abnormality in the mediastinum. For example, it may suggest mediastinal or hilar adenopathy. Narrowing or deviation of the tracheobronchial tree, enlargement of the pericardial silhouette, and calcification or enlargement of the great vessels are other abnormalities that may initially be seen radiographically (Fig. 42-1A). However, because of its limited resolution, the chest film often does not provide adequate information about specific mediastinal pathology. Further radiographic assessment by other modalities is necessary for a more accurate assessment.
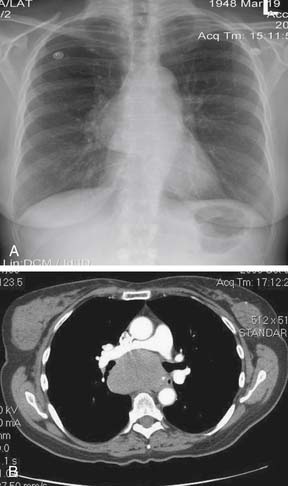
Computed tomography (CT), often with intravenous or oral contrast, is indicated when mediastinal pathology is suspected on the basis of the chest film (see Fig 42-1B) or clinically. High-resolution spiral CT, with cross-sectional imaging of structures at intervals as narrow as 1 mm, is the radiologic modality of choice for imaging the middle mediastinum. All structures located in the middle mediastinum can be seen by CT. In addition, the relationship of these structures to other nearby structures can be delineated. Three-dimensional CT images can be reconstructed using computerized programs without the need for additional radiation. These reconstructions can be particularly useful for detailed assessment of structures, such as the trachea, located in the middle mediastinum.
Positron emission tomography (PET) is a valuable tool for evaluating mediastinal pathology, especially mediastinal lymph node involvement in neoplasms (e.g., lung cancer). The degree of uptake of fluorodeoxyglucose (FDG) labeled with radioactive fluoride (18F) is a surrogate marker of the degree of metabolic activity in a cell. However, PET is limited, because it is difficult to distinguish between increased metabolic activity caused by tumor and that caused by inflammation. Furthermore, as PET does not provide an anatomic scan, the precise location of the increased metabolic activity may not be discernable. However, fusion of PET with CT (CT-PET) has allowed a more precise assessment of anatomy.1
Conventional ultrasonography is of limited value in the evaluation of middle mediastinal pathology, although it may help in determining whether a mass is cystic or solid. However, transesophageal endoscopic ultrasonography (EUS) has emerged as a valuable tool for the evaluation of certain mediastinal pathology, especially lymph nodes.2 Other modalities, such as leukocyte scintigraphy, lymphoscintigraphy, and metaiodobenzylguanidine (MIBG) scanning, have limited and very specific indications in the evaluation of pathology in the middle mediastinum.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


