In a 63-year-old man, episodes of ventricular tachycardia causing syncope and myocardial infarction are the first manifestations of triple vessel coronary disease in the absence of arteriographic evidence of a fresh occlusion.
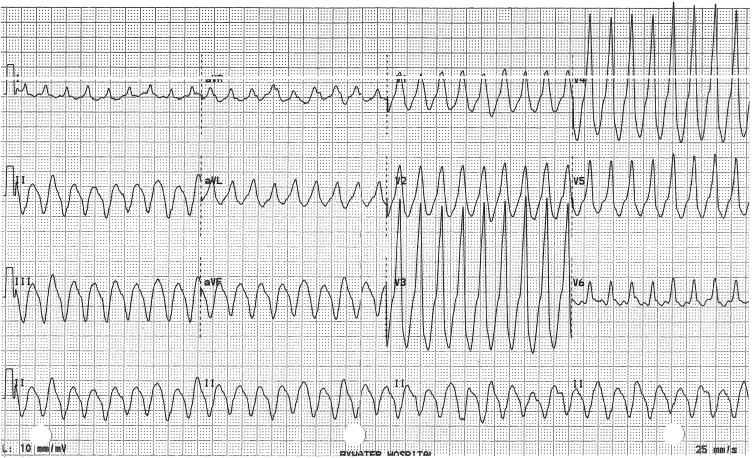
While working outside on a hot summer day, a 63-year-old man went inside an even hotter shed for a tool and had a syncopal episode. When he regained consciousness, he was dyspneic and had epigastric and lower anterior chest pain. He again felt weak, could not stand, had difficulty dialing the phone for help, and had an involuntary bowel movement. In a local hospital’s emergency department, an electrocardiogram was recorded ( Figure 1 ), and after ineffectually striking him on the chest anteriorly, a nurse electrically cardioverted him.
The initial electrocardiogram showed a monomorphic ventricular tachycardia at a rate of 214 beats/min. Many features of this wide QRS tachycardia confirmed that it was ventricular tachycardia. The QRS morphology was unlike that of right or left bundle branch block. None of the V leads had an RS complex. The left peak of the R wave in lead V 1 was taller than the right peak. The QRS was exceptionally wide (0.21 seconds). No definite P waves, fusion complexes, or capture beats were identified, but at a ventricular rate above 200 beats/min that was not surprising. Although not quite as diagnostic as negative concordance, the positive precordial QRS concordance strongly suggested ventricular tachycardia, especially in this clinical setting and with a history of systemic arterial hypertension, hyperdipidemia, heavy cigarette smoking (3 packs/day only recently down to 1 pack/day), and chronic obstructive pulmonary disease for which he had been using an inhaler.
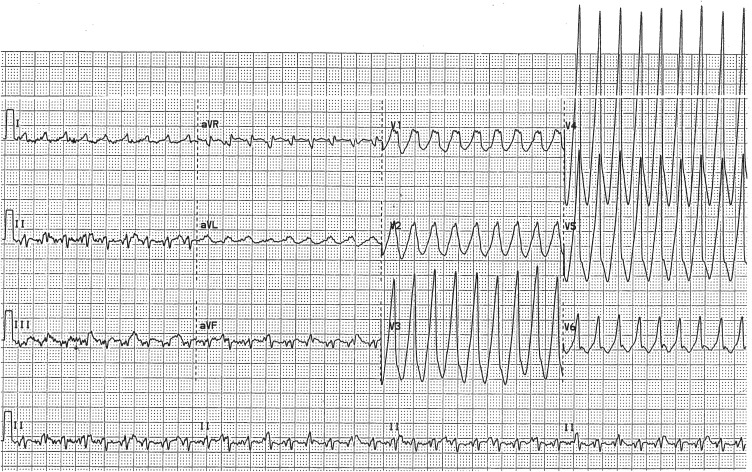
Over the next 2 days, the patient had further episodes of ventricular tachycardia ( Figure 2 ). Each time sinus rhythm was restored, transient, striking ST-segment depression in 8 to 10 leads and ST elevation in lead aVR signified extensive left ventricular ischemia/injury ( Figure 3 ). The serum troponin I level peaked at 125 ng/ml; reference, <0.04.