Synchronous Lung Nodules
Presentation
A 65-year-old woman presents for preoperative evaluation for elective knee replacement. The patient suffers from arthritic degeneration of her right knee and is severely limited in her ability to walk without pain.
Her past medical history includes hypertension and diabetes. She is a long-time smoker of 30 pack-years, but quit 10 years ago. She denies chest pain and shortness of breath, but she is limited in her activity because of her arthritis. She denies weight loss.
On physical examination, the patient is in no acute distress. Her pulse is 80 beats/min, and her blood pressure is 100/60 mm Hg. She has no cervical adenopathy. There are normal breath sounds heard upon auscultation of her chest, and her cardiac examination reveals only a displaced point of maximal impulse (PMI). The right knee is enlarged and somewhat tender and has a limited range of motion.
As part of her preoperative evaluation, routine chemistries and hematologic profiles are drawn and found to be normal. Chest x-rays are performed.
▪ Chest X-rays
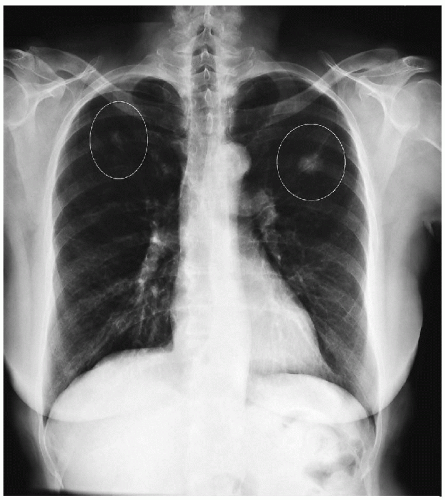 Figure 43-1 |
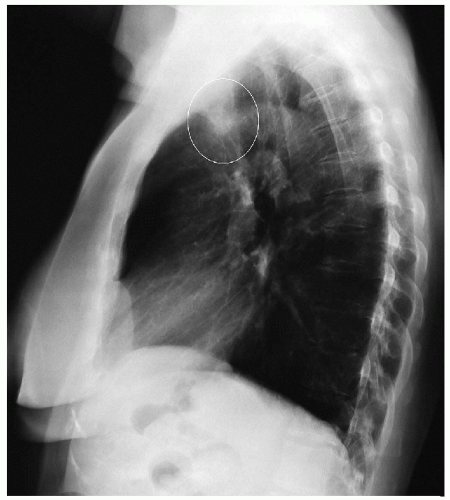 Figure 43-2 |
Chest X-ray Report
Two nodules are present in both lung fields. One nodule is in the left upper lobe, and one is in the right upper lobe. The heart is not enlarged. There are no pleural effusions.
Discussion
Primary lung cancer, metastatic carcinoma, sarcoma, hamartoma, carcinoid, tuberculosis, and histoplasmosis should be considered in this patient. A computed tomography (CT) scan will provide further anatomic localization as well as evaluate the mediastinum for enlarged lymphadenopathy. A positron-emission tomography (PET) scan can also be obtained to evaluate for metastatic disease.
▪ CT Scans
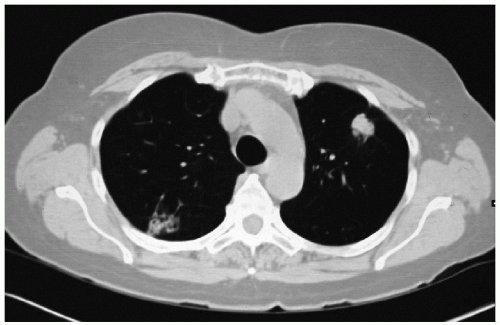 Figure 43-3 |
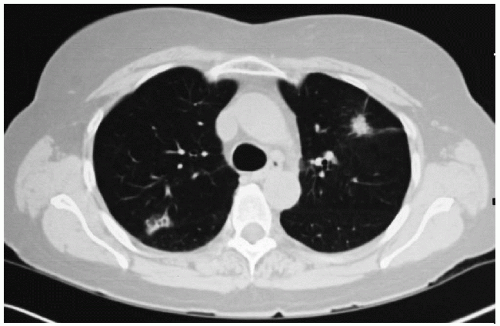 Figure 43-4 |
CT Scan Report
CT scans demonstrate a 2.0-cm mass in the anterior segment of the left upper lobe and a 2.5-cm mass in the posterior segment of the right upper lobe. No adenopathy is noted in the mediastinum.
▪ PET Scans
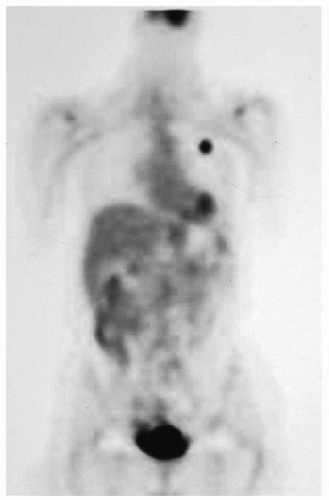 Figure 43-5
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|