This study investigated the long-term impact of the 2011 Japan earthquake and tsunami on the incidence of acute decompensated heart failure (HF) in the disaster area. This was a population-based study using comprehensive registration for all hospitals within the study area. The standardized incidence ratio (SIR) and 95% confidence interval (CI) for new onset of HF during the disaster year (2011) and postdisaster years (2012 to 2014) were determined. When SIR were compared between the low- and high-impact areas, as defined by the extent of tsunami inundation in residential areas, SIR showed a significant increase in high-impact areas in 2011 (1.67, 95% CI 1.45 to 1.88) and tended to return to baseline in 2012, the first postdisaster year (1.25, 95% CI 1.06 to 1.43). The rate again increased in 2013 (1.38, 95% CI 1.18 to 1.57) and 2014 (1.55, 95% CI 1.35 to 1.75). In low-impact areas, no such increase was apparent during either the disaster year or the postdisaster years. Mean postdisaster period SIR for municipalities significantly correlated with the percentage of tsunami flooding in residential areas ( r = 0.52, p <0.05) and with the percentage of refugees within the population ( r = 0.74, p <0.01). There was no significant relation between maximum seismic intensity and mean SIR in these municipalities. In conclusion, these results suggest that the catastrophic tsunami but not the earthquake per se resulted in a prolonged increase in the incidence of HF among the general population living in tsunami-stricken areas.
Previous studies have reported a short-term increase in the incidence of acute cardiovascular events such as acute myocardial infarction and sudden cardiac death after major earthquakes and devastating storms. In terms of acute decompensated heart failure (HF), we have previously reported that the number of HF admissions in the tsunami-stricken area in our prefecture doubled and reached a peak several weeks after the 2011 northeast Japan earthquake and tsunami (which occurred on March 11, 2011), with admission levels returning to baseline within 2 months. In the same disaster, the number of ambulance transfers for possible patients with HF in the adjoining prefecture doubled immediately after the disaster and remained high for several weeks. Few studies have examined the long-term effect on the incidence of HF after combined disasters such as an earthquake and subsequent tsunami. This study, which used comprehensive registration across the entire study area, examined the impact of the devastating 2011 earthquake and tsunami on the incidence of cardiovascular events, specifically HF.
Methods
The study area included the coastal and inland areas of Iwate prefecture in northeast Japan ( Figure 1 , left ). According to national census data, the population of the study area was 334,500 in 2010 before the disaster. The area comprises 16 municipalities, and the percentage of elderly (age ≥65 years) in the area was 32% before the disaster.
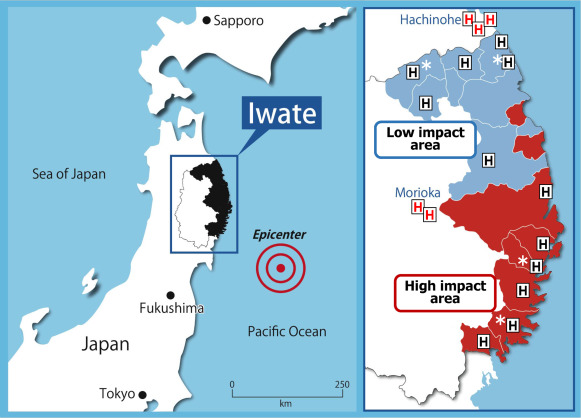
As in our previous report, to elucidate the effects of the tsunami on HF events, each municipality was categorized as either a low- or high-impact area according to the degree of tsunami inundation ( Figure 1 , right ). This definition was based on the percentage of tsunami flood area per built up area (TFA) in each municipality. This ratio represented the degree and extent of damage caused by the tsunami in residential areas of each town. The low-impact area was defined as TFA <10% or a remote area without a coastline, and the high-impact area was defined as TFA ≥10%. The low-impact area comprised 8 municipalities with a population of 129,800 in the predisaster years (2009 to 2010), with a gradual decrease to 121,600 in 2014. The high-impact area comprised 8 municipalities with a population of 206,300 in predisaster years, with a rapid decrease after the disaster to 184,700. In both areas, there were 6 general hospitals, with 2 of those having a cardiology department. Patients with decompensated acute HF were mostly admitted to the hospitals which had a cardiology department. General practitioners in the study area did not provide any care for patients with serious acute cardiac events.
In terms of maximum seismic intensity in these municipalities, there was no significant difference in scale between the low- and high-impact areas (4.6 ± 0.4, n = 8 vs 5.0 ± 0.6, n = 8; p = 0.11). The number of deaths on the day of the disaster was 12 in the low-impact area and 5,898 in the high-impact area. The number of evacuees in community centers or school gymnasiums at 1 month after the disaster (April 10, 2011) was 386 in the low-impact area and 42,880 in the high-impact area.
As completeness of case ascertainment is an important prerequisite for reliable analysis and estimation of trends for the incidence of cases in a particular area, the registry system in the present study was planned so as to capture all cases of decompensated acute HF in the study area by covering all hospitals in the study area. To ensure that as many as possible appropriate cases were identified, we visited all operating hospitals within the study area (n = 12) and 5 high-level hospitals outside the study area (Morioka and Hachinohe; Figure 1 , right ) and retrospectively reviewed medical charts and/or discharge summaries for patients in cardiology and internal medicine wards and emergency rooms.
The study team included cardiologists and trained research nurses who checked medical charts and registered all hospitalized cases with HF that met Framingham diagnostic criteria. Approval was obtained from the ethics review board of each participating hospital and Iwate Medical University before commencement of the study.
The present study examined the incidence (new onset) of decompensated acute HF in the study area from the date of the disaster (March 11, 2011) until the end of the postdisaster period (December 31, 2014). In addition, cases of HF for the corresponding periods in 2009 and 2010 were also surveyed to act as a time control. Patients who had been transferred to another hospital were counted on the admission index only. The standardized incidence ratio (SIR) and 95% confidence interval (CI) for HF during the disaster year (2011) and the following postdisaster years were determined respectively from the number of observed cases relative to the number of expected cases calculated by age adjusted by incidence for 2 predisaster years (2009 and 2010). Postdisaster SIR were compared between the low- and high-impact areas. Continuous variables are expressed as mean ± SD. Trend analysis among before- and after-disaster groups are based on the Cochran–Armitage test for trend. Pearson correlation coefficients were used to examine relation between mean SIR for the postdisaster period (2011 to 2014) and the percentage of TFA or the percentage of evacuees within each municipality population. A p value <0.05 was considered statistically significant.
Results
In the high-impact area, approximately 6,000 people (3% of the population) drowned or were missing on the day of the tsunami. This sudden population decrease was followed by a progressive decrease and reached approximately −10% of the initial population level in 2014, which was used for comparison with the predisaster level. In the low-impact area, the population gradually decreased to approximately −6% of the predisaster population level in 2014.
For clinical characteristics of HF, the percentage of elderly people (aged >75 years) and the percentage of men did not change during the study period in both low- and high-impact areas ( Table 1 ). In the low-impact area, the percentage of atrial fibrillation among HF cases was stable. In the high-impact area, the percentage gradually but significantly decreased during the study period (p for trend <0.001). In cases evaluated using 2-dimensional transthoracic echocardiography (83%), secular trend for the percentage of preserved left ventricular ejection fraction of ≥50% did not change in both study areas. For in-hospital mortality, there were no significant differences during the study period in either area.
| Variables | Pre-disaster 2009-2010 ∗ | Disaster 2011 | Post-disaster 2012 | Post-disaster 2013 | Post-disaster 2014 | p for trend |
|---|---|---|---|---|---|---|
| Overall area | ||||||
| number of case | 280 | 384 | 318 | 371 | 380 | |
| age ≥ 75yrs | 73% | 77% | 76% | 70% | 77% | 0.93 |
| men | 48% | 46% | 48% | 45% | 48% | 0.96 |
| atrial fibrillation | 56% | 58% | 52% | 43% | 51% | <0.01 |
| left ventricular EF ≥ 50% | 49% | 47% | 45% | 48% | 50% | 0.61 |
| in hospital mortality | 13% | 10% | 12% | 12% | 9% | 0.33 |
| Low-impact area | ||||||
| number of case | 137 | 156 | 145 | 176 | 156 | |
| age ≥ 75yrs | 76% | 77% | 79% | 72% | 83% | 0.45 |
| men | 45% | 46% | 44% | 44% | 46% | 0.95 |
| atrial fibrillation | 55% | 54% | 54% | 44% | 57% | 0.63 |
| left ventricular EF ≥ 50% | 50% | 49% | 45% | 44% | 46% | 0.30 |
| in hospital mortality | 10% | 10% | 12% | 13% | 11% | 0.60 |
| High-impact area | ||||||
| number of case | 143 | 228 | 173 | 195 | 224 | |
| age ≥ 75yrs | 70% | 76% | 75% | 69% | 72% | 0.62 |
| men | 51% | 46% | 51% | 46% | 50% | 0.99 |
| atrial fibrillation | 56% | 60% | 51% | 43% | 46% | <0.001 |
| left ventricular EF ≥ 50% | 48% | 46% | 45% | 52% | 52% | 0.21 |
| in hospital mortality | 16% | 9% | 12% | 11% | 8% | 0.09 |
Temporal changes in SIR (95% CI) in the overall area were 1.40 (1.26 to 1.54) in 2011, 1.14 (1.01 to 1.26) in 2012, 1.30 (1.17 to 1.44) in 2013, and 1.31 (1.18 to 1.44) in 2014. When the SIR was separately analyzed according to the degree of TFA (≥10% vs <10%), in the high-impact area, SIR significantly increased in the disaster year (1.67 [1.45 to 1.88] Figure 2 , left ). In the first postdisaster year (2012), SIR showed a trend to return to baseline (1.25 [1.06 to 1.43]); however, the ratio again increased in 2013 (1.38 [1.18 to 1.57]) and further increased in 2014 (1.55 [1.35 to 1.75]). In contrast, in the low-impact area, SIR was stable and did not show a significant elevation throughout the study period except for 2013 (1.21 [1.03 to 1.39]; Figure 2 , right ). Mean SIRs for the postdisaster period (2011 to 2014) were calculated for each municipality and compared with the percentage of TFA or the percentage of refugees evacuated to community centers or school gymnasiums at 1 month after the disaster in each municipality population. SIR for HF events significantly correlated with several parameters related to tsunami damage (%TFA: r = 0.52, p <0.05; %evacuees: r = 0.74, p <0.01; Figure 3 ). There was no significant relation between maximum seismic intensity and mean SIR (2011 to 2014) in these municipalities ( r = 0.27, p = 0.32).



