Surgery for Mechanical Complications of Myocardial Infarction
The mechanical complications of acute myocardial infarction have serious clinical implications and are generally associated with a poor prognosis. The onset of ischemia is usually heralded by pain that may be followed by shock and ventricular failure owing to significant myocardial injury. The severity of symptoms and clinical manifestations are intimately related to the magnitude of myocardial necrosis and loss of contractile strength.
Necrosis of the free ventricular wall may cause acute myocardial rupture. Necrosis of the ventricular septum may result in an acute septal defect and sudden left-to-right shunt leading to hemodynamic instability. Necrosis of papillary muscles will result in papillary muscle dysfunction or rupture causing severe mitral valve insufficiency.
Patients are initially stabilized with medical management and intraaortic balloon counterpulsation before undergoing cardiac catheterization and coronary angiography. Most of them will require emergent surgery because of intractable and progressive cardiogenic shock. Concomitant coronary artery bypass grafting should always be contemplated, whenever possible, to achieve complete myocardial revascularization. A small subgroup of these patients may compensate and present late with a pseudoaneurysm, left ventricular aneurysm, ventricular septal defect, or ischemic mitral valve insufficiency.
Exposure and Cannulation of the Heart
The heart is exposed through a median sternotomy. Venous drainage is accomplished through bicaval cannulation, although a single large atrial cannula is adequate whenever the right heart remains a closed system during the procedure. Arterial blood is returned by direct aortic cannulation.
When there is evidence of contained bleeding within the pericardium due to a pseudoaneurysm or rupture of the heart, it is prudent to cannulate the aorta through a small enough opening in the pericardium overlying the aorta to allow volume replacement during venous cannulation and initiation of cardiopulmonary bypass. Alternatively, femoral cannulation should be contemplated.
Most patients requiring surgical intervention for management of acute mechanical complications of myocardial infarction are in cardiogenic shock. Many may be on intraaortic balloon pump support. Cardiopulmonary bypass is initiated, and the heart is decompressed by a vent catheter introduced into the main pulmonary artery or through the right superior pulmonary vein into the left ventricle. Core cooling to 30° to 32°C is carried out, and the aorta is clamped. Cold blood cardioplegic solution is then administered through the aortic root followed by retrograde delivery into the coronary sinus (see Chapter 3).
Acute Myocardial Rupture
Cardiorrhexis is a dramatic and lethal event. It is virtually always associated with a transmural infarction. Through a rent in the ventricular endocardium, blood gradually leaks into the area of infarction and distends the necrotic tissue. This hematoma continues to expand and finally ruptures the myocardium. The incidence of myocardial rupture after myocardial infarction is 10 times greater than either a ventricular septal defect or papillary muscle tear. The left ventricle is involved in 90% of all ruptures.
The sudden onset of cardiogenic shock 3 to 4 days after acute myocardial infarction may herald the development of cardiac tamponade due to myocardial rupture. Equalization of pressures in the right atrium, right ventricle in diastole, and pulmonary artery wedge, as measured with a Swan-Ganz catheter and aspiration of blood from the pericardial cavity are significant clues to the accurate diagnosis.
Immediate surgical exploration through a standard median sternotomy should be undertaken. If the heart has actually overtly ruptured, only a salvage operation may be successful. This entails prompt initiation of cardiopulmonary bypass. The infarcted necrotic tissue is removed. An appropriate patch of Hemasheild or bovine pericardium is sewn to the healthy normal myocardium
with a continuous suture of 3-0 Prolene buttressed with a strip of felt to cover the defect. The suture line may have to be reinforced with additional sutures.
with a continuous suture of 3-0 Prolene buttressed with a strip of felt to cover the defect. The suture line may have to be reinforced with additional sutures.
More commonly the rupture consists of a small rent in the myocardium. The infarcted segment becomes spongy, oozing with blood. At times there may be a small hole through which blood spurts out. This may be amenable to suturing a large patch to the surrounding normal myocardium without resecting any muscle. Surgical management of this type of myocardial injury has been simplified with the use of biocompatible glues, such as cyanoacrylate or histoacryl. The technique entails applying the glue to the relatively dried surface of the infarcted myocardium, and covering the area with an appropriately sized patch of Teflon felt or bovine pericardium. The procedure does not require cardiopulmonary bypass support, and can be performed expeditiously with improved patient survival.
 The sutureless technique for left ventricular rupture is a lifesaving procedure. Coronary artery bypass grafts are not performed, and generally these patients are taken directly to the operating room without undergoing coronary angiography.
The sutureless technique for left ventricular rupture is a lifesaving procedure. Coronary artery bypass grafts are not performed, and generally these patients are taken directly to the operating room without undergoing coronary angiography.Ventricular Septal Rupture
The ventricular septum receives blood from perforating branches of the left anterior descending artery as well as perforating branches of the posterior descending artery. Despite this dual blood supply, there is frequently no septal collateral flow. Consequently, the interventricular septum remains quite vulnerable to ischemia and occasionally ruptures after myocardial infarction. This is seen notably in patients whose infarction is the result of single-vessel disease. As with ventricular aneurysm, the anteroapical area is the most common site; it is involved in 65% of patients with ventricular septal rupture. The posterior segment of the septum is involved in 17% of the cases, and the middle segment in 13% of the cases; only 4% of the ruptures involve the inferior segment of the septum.
There is frequently a rapid progressive hemodynamic deterioration with myocardial failure following the rupture of the ventricular septum. The initial diagnosis is confirmed by echocardiography and is later followed by cardiac catheterization and coronary angiography. The goal of preoperative management is to decrease the left-to-right shunt by reducing systemic vascular resistance but at the same time ensuring adequate systemic blood pressure and cardiac output. Because these patients tend to die of end-organ failure rather than heart failure, prompt temporary stabilization is achieved with the support of an intraaortic balloon pump, ionotropic agents, and diuretics to maintain optimal tissue perfusion.
 At times it is possible to totally occlude the shunt with the balloon of the Swanz-Ganz catheter that has been passed across the septum, and stabilize the hemodynamics in preparation for subsequent surgical repair.
At times it is possible to totally occlude the shunt with the balloon of the Swanz-Ganz catheter that has been passed across the septum, and stabilize the hemodynamics in preparation for subsequent surgical repair.The operative mortality in this subgroup of patients is relatively high, but without urgent surgery, most of them would not survive.
Technique for the Surgical Treatment of a Ventricular Septal Defect
The septal defect is approached through an incision parallel to the course of the left anterior descending coronary artery in the center of the left ventricular infarct (Fig. 10-1). The septal defect and the extent of surrounding friable necrotic tissue are identified. With a continuous 3-0 Prolene suture, a generous patch of bovine pericardium is sewn to the left ventricular side of the septum, taking deep bites of normal, healthy muscular tissue as far away from the necrotic rim of the defect as possible. At times, this may necessitate sutures being placed close to the mitral valve annulus. The septal necrosis often extends to the ventriculotomy. The pericardial patch is then allowed to protrude outside the heart and be incorporated in the ventriculotomy closure (Fig. 10-2).
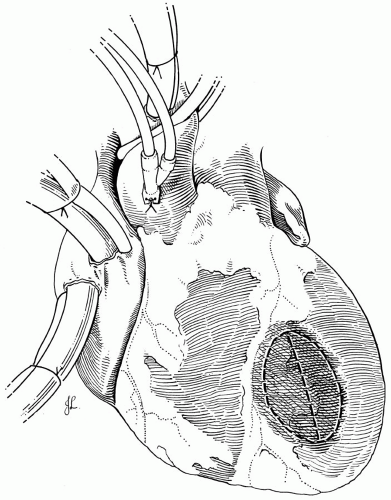 FIG 10-1. Technique for surgical treatment of a ventricular septal defect. |
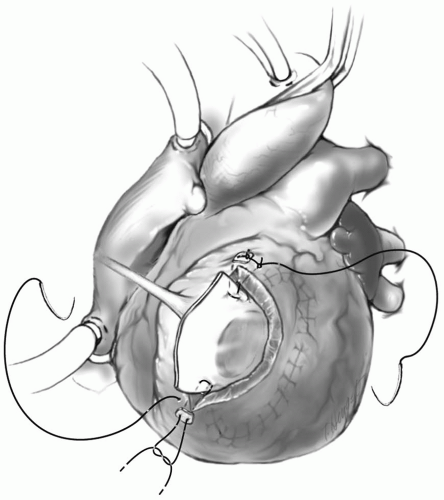 FIG 10-2. A generous patch of bovine pericardium is sewn to the normal septal wall away from the defect. |
 Bioglue Surgical Adhesive, (Cryolife, Inc., Kennesaw, GA) may be used to glue the patch to the septum before suturing it in place. This provides an added safeguard for the integrity of the repair.
Bioglue Surgical Adhesive, (Cryolife, Inc., Kennesaw, GA) may be used to glue the patch to the septum before suturing it in place. This provides an added safeguard for the integrity of the repair.This technique essentially excludes the infarcted area. The suture line on the septum is inspected and checked for any residual defects. It is reinforced with multiple interrupted sutures buttressed with felt pledgets. The patch is anchored to the anterior edge of the left ventricular wall with a felted suture. This technique is based on the concept that the higher left ventricular pressure will force the pericardial patch against the entire septum, thereby obliterating the septal defect. Because sutures are placed on the normal healthy tissue, well away from the necrotic edges, the repair should be secure.
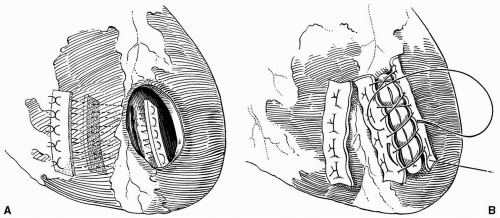 FIG 10-3. A: The slit-like ventricular septal defect is closed with interrupted sutures incorporating strips of Teflon felt on both sides of the septum and anterior wall of the right ventricle. B: The knots are then tied, and the ventriculotomy is closed. |
The ventriculotomy is then closed with interrupted sutures of 3-0 Prolene with a layer of Teflon felt strip on each side of the incision. This is reinforced with a continuous suture of 3-0 Prolene and Bioglue.
When the septal defect is a narrow, slit-like opening in close proximity to the anterior wall of the right ventricle, the sutures are first passed through a strip of Teflon felt, then through the viable septal tissue along the posterior edge of the defect, and again through another strip of Teflon felt on the right ventricular side of the septum (Fig. 10-3A). The sutures are brought out through the anterior wall of the right ventricle before they are passed through another strip of Teflon felt. Finally, the sutures are tied down, and the ventriculotomy is closed as described previously (Fig. 10-3B). Alternatively, the single pericardial patch technique could be used.
If the apex of the heart has infarcted and is necrotic, it is amputated. The viable tissue is then reapproximated in a sandwich manner by means of four strips of Teflon felt, one on each side of the septum and one each on the right and left exterior ventricular walls, with a series of interrupted horizontal mattress sutures (Fig. 10-4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


