Fig 1.
Simulation of reduced scan length and estimated organ doses in pulmonary CT angiography to rule out pulmonary embolism, in which the lung apex and base are excluded. A reduction of the effective dose by about one third compared with the original scan volume is estimated by the dose management software (Radimetrics, Bayer, Germany)
Positioning of the Arms
In thoracic CT, the patient’s arms should be raised over his or her head to achieve a dose-efficient thoracic CT scan with acceptable image quality. The increased attenuation by the arms in the x-axis forces the automatic tube current modulation to increase the radiation dose to maintain constant image quality thus increasing the radiation dose to most organs. Furthermore, with the arms next to the thorax, beam-hardening artifacts are increased degrading image quality (Fig. 2). Compared to arm-down positioning, placing the arms above the head increases subjective and objective image quality [8] and leads to a dose reduction of up to 45% in CT of the thorax and abdomen [9]. If a patient is unable to lift one arm, the technician should still position the other arm above the head.
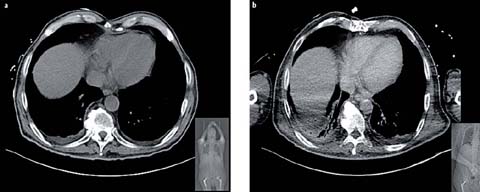
Fig 2 a, b.
Localizer radiograph and transverse CT slice of the lung base in a patient who underwent two CT examinations, one in which the arms were raised over the head (a) and the other with the arms placed next to the thorax due to immobility (b). The second CT scan resulted in an increase of beam hardening artifacts and reduced image quality in the lung bases
Patient Positioning in the Isocenter of the CT Scanner
The detrimental radiation dose effect of mis-centering patients within the scanner gantry is often not appreciated by technicians and radiologists. The increased radiation dose associated with mis-centering arises from the pre-patient X-ray beam bowtie filters installed in all modern CT scanners. These filters modify beam strength by strongly attenuating the peripheral projections and weakly attenuating central ones. This evens the X-ray fluence at the detector and reduces the radiation dose to less-attenuating peripheral structures. Incorrect centering defeats the purpose of the bowtie filter, leading to an increased radiation dose to peripheral structures and a decreased image quality [10]. Clinical studies have found that up to 95% of patients receiving a thoracic or abdominal CT scan are not centered properly in the vertical plane [10], with an average error of 2.6 cm. Li et al. quantified this effect, thereby demonstrating that a vertical mis-centering of 3 cm results in an increase in the peripheral radiation dose of up to 18%, with a 6% increase in image noise [10]. Thus, technicians should be trained to meticulously center patients such that the bowtie filters are utilized optimally.
Technical Advances for Dose Reduction
In the last 10 years, CT manufacturers have introduced a number of effective tools that reduce the radiation dose while maintaining or improving image quality. The clinical consequence of impaired image quality associated with dose reduction has been demonstrated in experimental studies using computer-simulated low-dose scans [11]. In the experimental design, intra-observer agreement was lower when noisy, low-dose rather than higher dose exams were interpreted [12]. The authors concluded that optimal dose reduction should be achieved without sacrificing image quality. Since CT manufacturers use diverse technical approaches for dose reduction, there are some differences in the technical implementations and their resultant effectiveness.
Automatic Tube Current Modulation
Since radiation dose is linearly related to tube current at constant kVp, a decrease in the tube current results in dose reduction. Although image noise is impacted by dose reduction, there is no impact on the CT numbers (Hounsfield units) of the body tissues scanned. The aim of automatic tube current modulation (ATCM) is to maintain operator-selected image quality throughout the scan while reducing the radiation dose to the patient. State-of-the-art ATCM modulates the tube current in three dimensions (x-,y-, and z-axes) for every slice of the scan, based on the X-ray attenuation within the slice. Tube current modulation is implemented based on either: 1. attenuation measurements obtained from the topogram or scout views: This approach is used by all manufacturers for z-axis (longitudinal) ATCM modulation, but is used by GE and Toshiba for the x– and y-axes (transverse or angular) [13, 14]; 2. tube current adjustment “on the fly” using the measured attenuation of the previous one-half gantry rotation: This approach is used by Siemens for x, y (transverse or angular) ATCM modulation [15].
The noise level or desired image quality is user-programmable and typically adjusted according to the clinical task specified on the clinical requisition. Therefore, the effectiveness of ATCM dose reduction is dependent on the radiologist. Each manufacturer uses a proprietary method to define the desired image quality (e.g., reference mA by Siemens, noise index by GE, standard deviation by Toshiba, reference images by Philips). In chest CT, a dose reduction of 20–26% can be achieved in average-size patients using ATCM rather than fixed tube current [16]. However, in very large patients, ATCM can result in increased radiation doses [17] because the system attempts to maintain uniform image quality almost independently of body size. Thus, the operator needs to be aware of this important caveat and to adjust the image quality level in obese patients.
A few years ago, organ-based tube current modulation was introduced by one manufacturer with the goal of reducing the tube current (x–y plane) when the X-ray tube was positioned over radiosensitive organs, including the female breast, the thyroid gland, and the lens of the eye. Long term follow-up data from the Life Span Study have shown that the radiation sensitivity of female breast tissue is higher than previously thought. Consequently, in the 2007 ICRP (International Commission on Radiological Protection) publication [18], the tissue weighting factor of the female breast was increased. Because in chest CT the breasts are included in the scan range but are not the target organ of the imaging procedure, it is important to decrease the radiation dose to these radiosensitive tissues. Organ-based tube current modulation reduces the tube current in the anterior 120° arc of the rotation by up to 25% of the tube current, while increasing the tube current to 125% over the remaining 240° of the rotation to maintain constant image quality in the center of the patient [19] (Fig. 3). In phantom studies, an average reduction of the breast dose up to 37% was achieved [20]. Nevertheless, recent clinical studies showed that in a majority of women (up to 99%) parts of the glandular breast tissue are located outside the dose-reduced sector and therefore might be at increased risk of overexposure when organ-based tube current modulation is used [20, 21]. Further refinement of this technique will be required to better protect radiosensitive breast tissue.
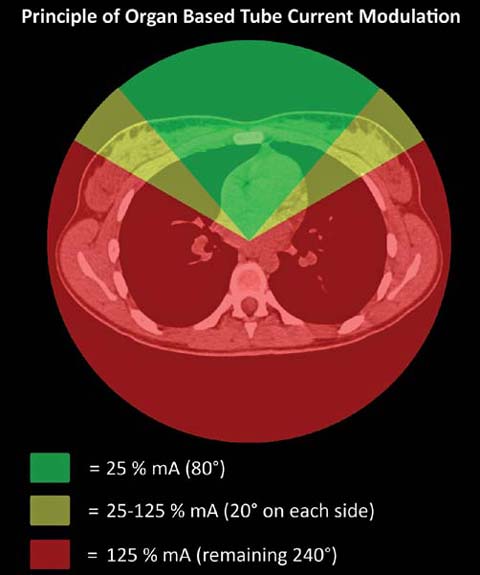
Fig 3.
Principle of organ-based tube current modulation: to protect radiosensitive organs such as the female breasts, the tube current is reduced during the anterior 120° of the gantry rotation. To maintain image quality in the center of the image, the tube current is augmented for the remaining 240° of rotation
Adjustment of the Tube Voltage for Pulmonary CT Angiography
Increasing attention is being paid to the use of lower tube voltages (80–100 kVp) in contrast-enhanced CT. In the chest, pulmonary CT angiography to rule out an embolism is well suited for a low tube voltage technique for two reasons (Fig. 4): while the radiation dose decreases at a more than linear rate, the iodine contrast enhancement increases substantially (by a factor of 2, for example, when the tube voltage is decreased from 140 to 80 kVp). The increased attenuation of contrast medium at reduced kVp (70–100) is secondary to the enhanced photoelectric effect at a lower kVp. Two publications demonstrated that image quality did not decrease when the peak tube voltage for pulmonary CT angiography was lowered to 100 kVp, while resulting in a dose reduction of up to 50% [22, 23]. Furthermore, Schueller-Weidekamm et al. reported an increase in analyzable segmental pulmonary arteries at 100 kVp compared to 140 kVp [23]. The first large-scale prospectively randomized study (REDOPED) investigating the accuracy of low-dose pulmonary CT angiography provided clear evidence that, in patients up to 100 kg body weight, an 80-kVp protocol yields very similar accuracy, diagnostic confidence, and image quality but with a dose that is 30% lower than in a 100-kVp protocol [24]. The estimated effective dose was only 2.25 mSv at 80 kVp. The study also suggested the potential for further dose reduction since it employed a dated CT technology using slow scan times and no iterative reconstruction.
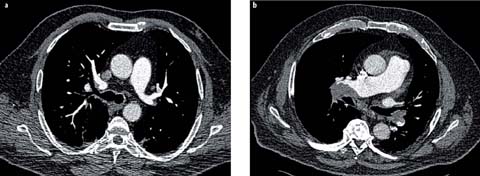
Fig 4 a, b.
Examples of lowering the tube voltage in pulmonary CT angiography to rule out pulmonary embolism. a A transverse slice in a male patient (95 kg body weight) who was scanned with 80 kVp [150 mA; volume CT dose index (CTDIvol) of 4.2 mGy]. b An obese male patient (150 kg body weight) scanned with 100 kVp (100 mA, CTDIvol of 9.3 mGy). Both images were acquired on a 16-slice MDCT scanner and reconstructed with filtered back projection. The images clearly demonstrate that, even with dated CT technology, lowering of the tube voltage in pulmonary angiography is possible without impairing diagnostic accuracy
Reduced tube voltage can be implemented either manually or using an automated technique. We employ a manual technique based on clinical observation and measurements; specifically, an 80-kVp protocol is applied for patients with a body weight up to 100 kg and a 100-kVp protocol for patients with a body weight >100 kg (Fig. 4). At least two manufacturers offer automatic tube voltage selection, which selects an optimal tube voltage based on patient size, selected CT protocol, and operator-defined image quality [25]. In a prospective study, Niemann et al. demonstrated a dose reduction of 39% in pulmonary CT angiography using automatic tube voltage selection [25]. Instead of the standard tube voltage of 120 kVp, in 28% of the cases a tube voltage of 100 kVp and in 69% of the cases a tube voltage of 80 kVp were automatically selected.
Iterative Reconstruction Technique
While the commonly used filtered back-projection image reconstruction technique is computationally efficient, it suffers from noise and artifact limitations. Despite their availability over 20 years ago, iterative reconstruction (IR) techniques never gained acceptance due to their computational intensity and slow image reconstruction speed. The advent of faster computer platforms and the demand for a reduction of the radiation dose without an increase in image noise has spurred research into IR. The nomenclature of IR techniques is not yet standard. Manufacturers have developed a number of proprietary techniques involving different strengths and varying in reconstruction speed spatial resolution, and image noise. In general, in IR an initial image is formed that is then used to generate simulated raw scan data, which are compared to the acquired scan data. A new image is then generated based on the difference. This process is repeated, or iterated to further improve the image. IR can operate either with image and raw scan data space (Adaptive Statistical Iterative Reconstruction, ASIR, GE Healthcare; Adaptive Iterative Dose Reduction 3D, AIDR 3D, Toshiba, Sinogram Affirmed Iterative Reconstruction, SAFIRE, Siemens Healthcare; and iDose, Philips Healthcare) or raw scan data space alone (MBIR or Veo, GE Healthcare; Advanced Modeled Iterative Reconstruction, ADMIRE, Siemens Healthcare). IR is a powerful tool to either improve image quality in large patients or to maintain diag-nostically adequate noise while decreasing radiation dose in small or intermediate sized patients.
There are numerous reports of substantial dose reductions using IR rather than standard filtered back projection while maintaining image quality [26, 27]. However, radiologist applying IR techniques have to be aware of the fact that images thus reconstructed tend have a blotchier and more pixilated appearance, impacting the evaluation of normal anatomic lung structure such as the interlobular fissures, subsegmental bronchial walls, and small peripheral blood vessels [27]. This occurs particularly with very aggressive noise reduction in order to achieve sub-mSv chest CT scans. Moreover, the image quality of sub-mSv chest CT is suboptimal for diagnosing mediastinal structures such as lymph nodes [27]. In the use of IR techniques for dose reduction in general, radiologists are advised to pay extra attention to the diagnostic accuracy with respect to the detection of small pulmonary nodules on the IR images. This advice is given against the background of the substantially decreased image noise achieved with IR but no impact of improved lesion detectability [28].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


