influence the absolute time periods of salvage ability (collaterals, intermittent occlusion, myocardial oxygen consumption, ischemic preconditioning, persistence of residual blood flow, recruitment of collaterals, hibernating). Time-independent benefits of opening the artery have also been suggested to exist, and include improving infarct healing, electrical stability, and reducing in reinfarction.
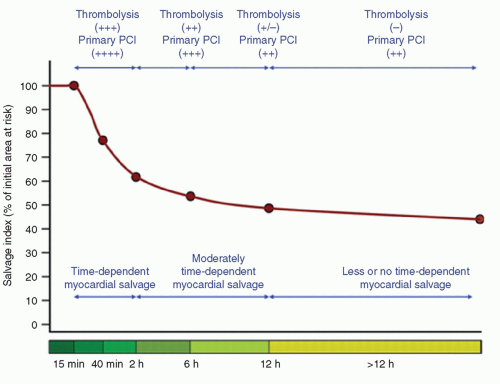 FIGURE 17-1 Time dependency of myocardial salvage expressed as percentage of initial area at risk. The initial parts of the curve up to 2 hours were reconstructed based on the experimental studies. For the first 15 minutes after coronary occlusion, myocardial necrosis is not observed. At 40 minutes after coronary occlusion, myocardial cell death develops rapidly, and the myocardial necrosis is confluent. After this point, progression to necrosis is slowed considerably. The other parts of the curve showing myocardial salvage from 2 to >12 hours from the symptom onset are reconstructed according to the data of scintigraphic studies in patients with acute myocardial infarction. Efficacy of reperfusion is expressed as follows: ++++, very effective; +++, effective; ++, moderately effective; ±, uncertainly effective; —, not effective. (From: Schömig A, et al. Eur Heart J. 2006;27:1900-1907, with permission.) |
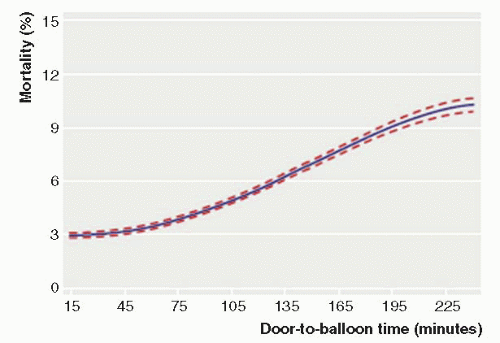 FIGURE 17-2 Adjusted in-hospital mortality as function of door-to-balloon time. Median D2B time was 83 minutes, with 4.6% mortality. Longer door-toballoon times were associated with a higher adjusted risk of mortality in hospital in a continuous nonlinear fashion (30 minutes = 3.0%, 60 minutes = 3.5%, 90 minutes = 4.3%, 120 minutes = 5.6%, 150 minutes = 7.0%, 180 minutes = 8.4%, p < 0.001). A reduction in door-to-balloon time from 90 to 60 minutes was associated with 0.8% lower mortality, and a reduction from 60 to 30 minutes with a 0.5% lower mortality. Data were from 43,801 STEMI patients undergoing primary PCI in NCDR (2005-2006). (Modified from: Rathore SS, et al. BMJ. 2009;338:b1807, with permission.) |
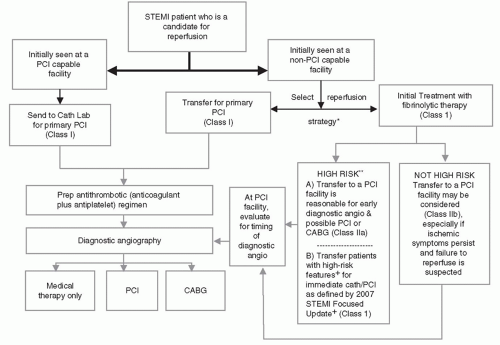 FIGURE 17-3 Guideline recommendations for triage and transfer for PCI in STEMI. Angio, angiography; CABG, coronary artery bypass graft; Cath Lab, catheterization laboratory; LOE, level of evidence; PCI, percutaneous coronary intervention; and STEMI, ST-segment elevation myocardial infarction. *Decision depends on multiple clinical observations including: Time since onset of symptoms; risk of STEMI; risks associated with fibrinolytic therapy; time required for transport to a skilled PCI laboratory. **High risk was defined in the CARESS-in-AMI (15) and the TRANSFER-AMI (14) studies. In CARESS-in-AMI, STEMI patients with at least 1 high-risk feature: extensive ST-segment elevation, new-onset left bundle-branch block, previous MI, Killip class ≥2, or left ventricular ejection fraction ≤35%. In TRANSFER-AMI, STEMI patients with ≥2 mm of ST-segment elevation in 2 anterior leads or ST elevation of at least 1 mm in inferior leads with at least 1 of the following: systolic blood pressure <100 mm Hg, heart rate >100 bpm, Killip class II to III, ≥2 mm of ST-segment depression in the anterior leads, or ≥1 mm of ST elevation in right-sided lead V4 indicative of right ventricular involvement. + In certain patients with high-risk features, a strategy of coronary angiography with intent to perform PCI is useful, regardless of the time since initiation of fibrinolytic therapy. These features include (a) Cardiogenic shock (provided suitable candidates for revascularization) (Class I recommendation for <75 years, Class IIb for age >75 years); (b) Severe congestive heart failure and/or pulmonary edema (Killip class III or IV); and (c) Hemodynamically compromising ventricular arrhythmias (Class IIa: patients >75 years and are in shock, hemodynamic, or electrical instability). (Adapted from: Kushner FG, et al. Circulation. 2009;120:2271-2306, with permission.) |
Primary PCI should be performed in fibrinolytic-therapy-ineligible patients who present with STEMI within 12 hours of symptom onset.
Primary PCI should be performed as quickly as possible, with a goal of medical contact-to-balloon (door-to-balloon) time of within 90 minutes.
If the symptom duration is within 3 hours and the expected door-to-balloon time minus the expected door-to-needle time is within 1 hour, primary PCI is preferred. However, if this duration is >1 hour, fibrinolysis is generally preferred.
Primary PCI should be performed for patients younger than 75 years with STEMI or new left bundle branch block (LBBB) who develop shock within 36 hours of myocardial infarction (MI) and are suitable for revascularization.
Primary PCI should be performed in patients with severe CHF and/or Killip Class 3 and onset of symptoms within 12 hours.
TABLE 17-1 Triage and Transfer Decisions for Reperfusion: Recommendations for STEMI Systems of Care | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 17-2 Indications for Coronary Angiography in ST-Segment Elevation Myocardial Infarction | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
In the absence of contraindications, fibrinolysis should be administered to STEMI patients with symptom onset within the prior 12 hours and ST-elevation >0.1 mg in at least two contiguous precordial leads or at least two adjacent limb leads.
In the absence of contraindications, fibrinolysis should be administered to STEMI or new LBBB patients with symptom onset within the prior 12 hours.
TABLE 17-3 Indications for PCI in STEMI | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
TABLE 17-4 PCI with or without On-Site Surgery: Recommendations | ||
|---|---|---|
|



