Radiation therapy approaches remain the cornerstone of management for patients with stage IIIB advanced non-small cell lung cancer (NSCLC). Radiation therapy alone, however, is today only rarely given as a single treatment modality. Historically, combined modality trials have demonstrated that induction chemotherapy prior to radiation already improves long-term results by improvement of systemic control.1,2 Progress has been made significantly with concurrent application of platinum-based chemotherapy to radiation treatment. This concurrent chemoradiotherapy strategy significantly increases local control and thus long-term results. At this time point, a concurrent chemoradiotherapy strategy—whenever possible—represents the standard of care for a large number of patients in this stage.3 Platinum-based combinations have emerged as typical partners of radiation, but adequate coverage of systemic risks of the patients has to be taken into account. Different strategies have either tried to give consolidation chemotherapy following a combined chemoradiation protocol. An alternate possibility looks at an induction chemotherapy strategy followed by the definitive concurrent chemoradiation protocol. The optimal combination strategy has not yet been established so far. The reader will learn to evaluate different multimodality regimens regarding their local and systemic efficiency. At the end of this chapter, the reader should in concert with the other chapters dealing with radiotherapy delivery and application be able to (a) learn that the patient population subsumed under the IIIB stage grouping represents a very heterogeneous patient group; (b) define the different risk factors of the individual patients including their local, locoregional, and systemic risks; (c) identify the small group of patients in whom surgery still represents a valuable strategy to include in this disease subset (e.g., T4N0 to N1); (d) group comorbidity profiles of the patients concerning their impact and relevance on the choice of the treatment protocol; (e) be critically aware of the results with typical chemoradiation protocols based on either cisplatinum combinations as well as carboplatinum combinations; (f) know about the differences of radiation delivery protocols including different dosing schedules as well as dose fractionation issues; (g) learn that new ways to improve this treatment design include a possible integration of molecular-targeted agents into this setting of definitive chemoradiation; (h) identify the toxicity profiles of typical definitive chemoradiation protocols both concerning their acute toxicities as well as possible late toxicities and their proper management; and (i) lead the interdisciplinary discussion in the individual patient based on his existing risks and define the aims of a multidisciplinary treatment strategy, including systemic treatments (medical oncology), radiation therapy, and surgery in selected cases. This knowledge of the possible pros and cons of individual treatment approaches will help to critically discuss these issues with the patient and finally, following this open discussion, generate an individualized treatment strategy for each patient. At the end of this chapter, the reader will also learn possible future innovative strategies to optimize the therapeutic management of patients with stage IIIB NSCLC.
HETEROGENEITY OF PATIENTS WITH STAGE IIIB NSCLC
The International Staging System includes into stage IIIB disease different patient groups with T4 tumors as well as involvement of contralateral mediastinal nodes at the N3 position.4 Permutations of these factors lead to different TN groupings—from T4N0 to T1N3 or even more unfavorable T4N3 categories. Recently, the proposals by the International Association for the Study of Lung Cancer (IASLC) staging committee have regrouped ipsilateral pulmonary metastases outside the involved lobe as stage T4 disease and ipsilateral pulmonary metastases inside the primarily involved lobe as T3 disease5 (see Chapter 30). Pleural effusion and pleural metastases are now considered to be M1 disease, thus reflecting the already known separation of this group outside of any combined modality approach including radiation therapy. The newly proposed stage groupings (especially the T4 subsets) have, so far, not been implemented into the clinical trials performed with multimodality treatment in NSCLC. Future trials for patients with stage IIIB should keep this in mind and should carefully give the individual subsets included into their patient selection. The T factor represents a very different number of clinical situations with important implications on possible surgical measures. T4 disease can include potentially resectable situations as involvement of the main carina, parts of the atrium, one or two segments of trachea, vertebral body, superior vena cava infiltration, or involvement of central parts of the pulmonary artery. Other subsets include those with esophageal, thoracic aorta, or extensive cardiac involvement. These represent definitively irresectable subsets. Even in the very few potentially resectable T4 indications, surgery is today usually performed within a clearly defined multimodality setting, taking care of the increased systemic risks of these patients. Besides the stage groupings and subsets, different other prognostic factors should be recognized for these patients, but some of them are not well defined yet (Table 56.1).6 These include histopathology (e.g., neuroendocrine, rare histopathological subsets) or tumor differentiation (G3 vs. G1), serumlactate dehydrogenase (LDH) as an unspecific marker of tumor burden, gender (female vs. male), performance status (0,1 vs. 2), pretreatment weight loss, and patient age. Besides prognostic factors, major comorbidities have to be taken into account for development of individual treatment plans. These include pulmonary function and significant pulmonary diseases (e.g., chronic obstructive pulmonary disease [COPD], emphysema, pulmonary hypertension), cardiovascular diseases (e.g., myocardial infarction, myocardial insufficiency), cardiovascular diseases (e.g., cerebral infarction), peripheral vascular problems, or other major organ dysfunctions (renal insufficiency, hepatic insufficiency, etc.). With most patients with lung cancer being at the age older than 60 years, these factors represent significant influences for the decision making in the individual patient. A valid denominator to make the comorbidity profiles of the patients objectively measurable are different Geriatric Assessment Scores in clinical use such as the Charlson Comorbidity Index.7 Thus, a significant heterogeneity of the patient population with stage IIIB is the natural consequence. Besides impact on potential operability of patients, comparable criteria exist concerning eligibility to intensive, definitive chemoradiation protocols, and administration of effective platinum-based chemotherapy regimen. With chemotherapy, radiotherapy, and (rarely) surgery being the major partners in multimodality treatment approaches, significant experience with handling of these modalities requires multidisciplinary treatment groups based on medical oncologists, pulmonologists, and radiation oncologists together with dedicated lung cancer surgeons. With increasing experience in the dedicated treatment center, toxicities and adverse effects of treatment can be significantly reduced, last but not the least from learning effects over time.
TABLE 56.1 Factors with Potential Influence on Prognosis of Patients with Stage IIIB NSCLC
Impact of Diagnostic Investigations to Define Different Subsets and Risk Groups in Stage IIIB
The small subset of patients with stage IIIB in whom surgery is being considered (T4N0) is typically staged extensively including thoracic computed tomography (CT) scans with vascular imaging studies based on adequate contrast media bolus-tracking techniques. Recently, positron emission tomography (PET) scanning has become an important addendum to the staging investigations, mainly for ruling out systemic metastases as well as mediastinal lymph node involvement.8 Cervical, parasternal, or extended mediastinocopy are typically performed to rule out extensive mediastinal lymph node involvement (N2, N3) that represents a major adverse prognostic factor in this patient group.9 It can be used to verify positive findings from PET studies, and sometimes thoracoscopic techniques may be added to clarify unequivocal findings from imaging investigations. Recently, endoscopic ultrasound techniques (EUS) or endobronchial ultrasound techniques (EBUS) have become an interesting alternative to extend initial staging investigations to pathologic staging of solid tumors and mediastinal and hilar lymph nodes based on fine-needle biopsies guided by ultrasound.10 However, these patients with intensive, surgically or endoscopically based staging investigations still represent a very selective and small subset of the population with stage IIIB. If definitive chemoradiation protocols with curative intent are planned, mostly imaging investigations only are performed including CT studies. This also holds true for most clinical phase II trials or phase III studies of multimodality treatment (chemoradiation) that will be mentioned and discussed later. Recently, PET and PET-CT investigations have been included into initial staging for a better definition of the treatment fields in three-dimensional (3D) radiotherapy treatment planning.11 Functional PET imaging studies may also be used for identifying response to multimodality treatment on induction protocols but with limited impact once radiation therapy is included into the protocol.12 Inflammatory and stromal response to radiation treatment significantly hamper interpretation of these investigations, especially during the postradiotherapy inflammatory pneumonitis phase. It is not yet clear, whether repeated EUS- or EBUS-guided biopsies during or following multimodality protocols may help to identify selected high-risk treatment groups or low-risk patient groups with improved prognosis following multimodality treatment. Furthermore, some investigators have proposed redo-mediastinoscopy following induction protocols to select patients with upfront involvement of the mediastinal nodes properly for definitive local treatment following their response to initial treatment.13,14
Surgical Indications in Selected Stage IIIB NSCLC Patients as Part of Multimodality Protocols
Biologically, patients with T4N0 stage of NSCLC represent a small but selective subgroup of patients in this stage with more locally invasive tumors and probably, a lower risk of distant metastases. This may be the background for improved results with extensive surgical approaches that have been reported within several small phase II trials in this setting. Here, we will only give the selection criteria typically used in some of the reported trials. Following extensive surgical staging that has excluded mediastinal lymph node involvement, the final aim is complete resection, which can be achieved by extensive surgical procedures including simple and intrapericardial pneumonectomies, sleeve pneumonectomies, bilobectomies, pericardectomies, cardiosurgical techniques for the left atrium, plastic vascular surgical techniques involving the pulmonary artery, its branches and superior vena cava, carinal resections, resections of one to two tracheal rings, or vertebral body resections. Long-term survival has been reported in all of these subgroups. Unfortunately, most of these clinical trials have not employed chemotherapeutic integration within induction or adjuvant treatment protocols. Some of the multimodality trials that have looked at induction chemotherapy and radiotherapy protocols also had T4N0 patients among their patient selection (Table 56.2) (Fig. 56.1). The largest ones are probably the Southwest Oncology Group (SWOG) 8805 study,15 the West German Cancer Center trial,16 an Italian study,17 and a Spanish study.18 They tested definitive surgery following chemotherapy or complex chemoradiation induction protocols. In the SWOG 8805 study, 19 patients were included with T4N0 to N1 tumors.15 A subset analysis showed that this group had an excellent median survival of 28 months. The West German Cancer Center Study included 10 patients with T4N0 to N1 treated with induction chemotherapy followed by chemoradiotherapy and definitive surgery.16 The median survival of this selected subgroup of patients was found to be 26.5 months with a 5-year survival rate of 37.5%. An Italian study looked at an induction chemotherapy only protocol of two cycles of cisplatinum-based chemotherapy in 43 patients with T4 disease, but this included patients with N0 as well as N1 and N2 nodal status.17 Four-year survival rates of this selected T4 group were 19.5%, proving that long-term survival is possible with aggressive induction and surgical strategies among these patient groups. In the phase II 9901 trial of the Spanish Lung Cancer Group, selected stage IIIA-N2 and T4N0-N1 tumors were included. Patients were treated by induction chemotherapy only, followed by surgical resection.18 Overall response rate was 56%. In the 67 patients with stage IIIB disease, complete resection was obtained in 29 patients (43.3%). Overall median survival time for T4N0 to N1 tumors was 16.8 months. For completely resected T4N0 to N1 patients, an impressive 5-year survival rate of 53.2% was obtained.
TABLE 56.2 Selected Phase-II Trials with Surgery as Part of a Combined Modality Approach to NSCLC Stage IIIB (T4, N3)
cc RT, concurrent radiotherapy; cl med, contralateral mediastinal; HF-RT, hyperfractionated accelerated RT; NR, not reported; PE, cisplatin and etoposide; PVblM, cisplatin and vinblastine and mitomycin; PGD, cisplatinum and gemcitabine and docetaxel; PT, cisplatinum and paclitaxel; PVblFU, cisplatin and vinblastine and 5-fluorouracil; R0, complete (R0-) resection; RT, radiotherapy; scl, supraclavicular.
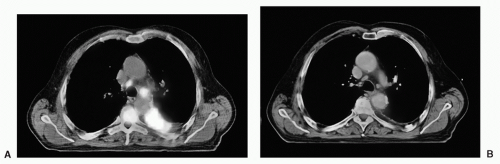
FIGURE 56.1 T4 disease with multimodality treatment including surgery. CT and PET/CT images of a patient with pathologically proven T4 disease at parasternal mediastinoscopy/thoracoscopy prior to induction treatment (A) and following an induction therapy (B) with induction chemotherapy (three cycles cisplatin and paclitaxel) followed by induction chemoradiotherapy (one cycle cisplatin and vinorelbine) with 45 Gy hyperfractionated accelerated radiotherapy (2 × 1.5 Gy bid). (See color plate.)
However, surgical intervention in T4N0 tumors with necessarily extended resections has significantly increased morbidity and mortality (>5%) rates if compared with simple lobectomies. Data on surgical management in selected N3 patients are even fewer (Table 56.2; Fig. 56.2). The SWOG 8805 included 27 patients with N3 disease in their induction chemoradiation trial, and the 2-year survival rate was 35% in the subgroup with supraclavicular N3 nodes but 0% in those with contralateral mediastinal nodes.15 The West German Cancer Center Group reported a larger series of 32 patients with N3 disease and found a median survival of 20 months with a 5-year survival rate of 28%.19 The Group in Paris aggressively treated 18 patients with N3 disease with induction chemoradiation followed by surgery and noticed a 17% 5-year survival rate. The surgical technique in this trial was a midline sternolaparotomy approach.20 The Cleveland Clinics Group treated 20 patients with proven N3 disease with an induction chemoradiation protocol including cisplatin, paclitaxel, and 30- to 33-Gy radiation.21 The 2-year survival rate to be observed was 15% in an early analysis. Typically, extended resections had to be performed, and in some trials contralateral mediastinal exploration was part of the operative procedure, whereas following complex chemoradiation protocols others did not explore the contralateral mediastinum at the time of thoracotomy. Surgical morbidity and mortality in all reported trials was increased compared with earlier disease stages. This has been the strongest argument against surgery in this setting, and it is generally accepted that this extensive surgery in the IIIB subset should be strictly performed in experienced hands in dedicated thoracic surgical centers. Furthermore, the number of patients treated in these trials was usually very small and also selective; therefore, a final evaluation of this concept is not possible. As no randomized trials are available, it is not clear whether the inclusion of surgery gives any benefit compared with definitive chemoradiation protocols that also have reported long-term survival outcomes in these stages.22
FIGURE 56.2 N3 disease with multimodality treatment including surgery. PET/CT images of a patient with mediastinoscopically proven N3 disease prior to induction treatment (A) and following an induction treatment (B) with chemotherapy (three cycles cisplatin and paclitaxel) followed by induction chemoradiotherapy (one cycle cisplatin and vinorelbine) with 45 Gy hyperfractionated accelerated radiotherapy (2 × 1.5 Gy bid). (See color plate.)
Historical Results of Radiation Therapy as Single Modality in Stage IIIB Those patient subsets with stage IIIB without pleural effusion or contralateral hilar lymph node involvement historically represented the group of patients primarily treated with radiation therapy alone in the 1980s and 1990s without any surgical intervention being possible. This local and locoregional approach already achieved a 5% to 7% long-term survival rate in selected patient populations.1,2 Radiation doses included were typically between 50 and 60 Gy over a 5 to 6 weeks’ application period. Over the years, with progress in radiation therapy delivery (electrons/photons with linear accelerators vs. Cobalt sources) and treatment planning (from two-dimensional planning with two or three treatment fields to 3D treatment planning based on CT studies), some benefit could be achieved with better efficacy versus toxicity profiles of the protocols (e.g., dermatological toxicity, radiation pneumonitis, cardiac toxicities, esophageal toxicities). The strongest argument against a single treatment modality in these locally far advanced stage IIIB patients comes from their relapse pattern. Within different clinical trials, between 40% and 70% of patients developed systemic relapses (systemic metastases to liver, bone, brain, adrenals, etc.), following the local modality only approach (surgery or radiation).1,2 This has been a major argument to introduce systemic treatment components such as chemotherapy into this setting.
Biological Rationale of Combining Chemotherapy Sequentially with Radiotherapy in Lung Cancer
Both chemotherapy and radiotherapy can theoretically have an effect on different tumor cell clones.23 Although radiotherapy exerts its effect on local and locoregional disease, chemotherapy may add significant effects on systemic micrometastases, besides a further activity on the primary tumor and its nodal involvement. Theoretically, this effect is most pronounced when both modalities are given separately in a sequential schedule as both modalities can be delivered without major dose and dose intensity compromises. The latter usually derive from overlapping or interacting toxicities once the modalities are combined at one time. These arguments have been the background for several clinical trials in stage III NSCLC patients looking at the sequential administration of chemotherapy and radiotherapy for stage III disease where IIIB patients were predominantly included.
Sequential Approaches of Chemotherapy and Radiotherapy in Comparison with Radiation Alone
Four prospective randomized clinical trials have looked at the sequential addition of induction chemotherapy to standard fractionated radiotherapy in stage III NSCLC (Table 56.3). All trials were multicenter trials and were performed on an intent-to-treat basis with upfront randomization. All four trials used cisplatinum-based combinations as induction therapy in the experimental arm and full cumulative radiotherapy doses between 56 and 65 Gy.
The Cancer and Leukemia Group B (CALGB) 8433 study compared a standard fractionated radiotherapy protocol of 60 Gy in 6 weeks or an experimental arm with cisplatin and vinblastine combination chemotherapy for two cycles as induction (Table 56.3).24 Patient selection included patients with good performance status and clinically staged IIIA and IIIB disease, usually low bulk lymph node involvement, and minimal weight loss. One hundred and fifty-five patients were randomized and there was a significant benefit in overall survival with 3-year survival rates of 24% versus 6% and 5-year survival rates of 17% versus 6% in favor of the induction arm (p = 0.012). Median survival was 13.7 months in the combined modality versus 9.6 months in the radiation only arm. Also, locoregional control was significantly improved with administration of the induction chemotherapy. No stratification was made for stage IIIB versus IIIA in this trial. The trial was prematurely closed based on positive findings at the first planned interim analysis and generated a first strong signal for the combined modality approach to stage III NSCLC patients.
TABLE 56.3 Randomized Prospective Multicenter Trials of Sequential Chemotherapy and Radiotherapy versus Radiotherapy Alone
Modified from: Eberhardt W, Pöttgen C, Stuschke M. Chemoradiation paradigm for the treatment of lung cancer. Nat Clin Pract Oncol 2006;3:188-199.
bid, twice daily; CALGB, Cancer and Leukemia Group B; NA, not applicable; NR, not reported; PE, cisplatin and etoposide; PVbl, cisplatin and vinblastine; RTOG, Radiotherapy Oncology Group; SLCSG, Scandinavian Lung Cancer Study Group; SplC, split course; S, survival; VCPC, vindesine, lomustine, cisplatin, and cyclophosphamide.
Based on the positive results of this trial, a subsequent North American Intergroup trial—initially Radiation Therapy Oncology Group (RTOG) trial 8808—tested the same induction therapy of two cycles of cisplatin and vinblastine induction followed by radiation therapy of the same 60 Gy against the radiation only arm.25 A third randomization arm of 69.9 Gy given in hyperfractionated application schedule (2 times 1.2 Gy bid) was added looking at a novel fractionation schedule of single-modality radiation therapy in this setting. No induction therapy was added in this intensified radiotherapy arm. With comparable inclusion criteria, this prospective randomized trial could confirm the benefit of induction chemotherapy followed by radiotherapy in this setting with a median survival of 17 months in the combined modality arm versus 11 months in the radiotherapy-alone arm (p = 0.04). However, 5-year survival rates were only marginally improved of 8% with the combination versus 5% in the radiotherapy-alone arm. No significant benefit was derived from the hyperfractionated radiotherapy application in the third arm. Critical voices following the publication of this trial argued that the low-single-fraction dosing of 1.2 Gy may be suboptimal, and one of the reasons for this failure to improve radiotherapy technique with this application schema.
The third study was performed in France as a multicenter randomized trial under the leadership of the Institute Gustave Roussy.26 Three hundred and thirty-two patients were prospectively randomized to receive a rather uncommon induction chemotherapy protocol based on cisplatin and vindesine in combination with cyclophosphamide and lomustine (VCPC)— a combination chemotherapy protocol developed and popular in France at that time—followed by 65-Gy standard fractionated radiotherapy. The standard arm was based on 65-Gy single-modality radiation treatment alone. An important and unique addendum to the trial were predefined bronchoscopic reinvestigations looking at the local control induced in the two treatment arms. There was a significant improvement in overall survival with 3-year survival rates of 13% with induction therapy versus 4% in the standard arm, and a 5-year survival rate of 6% versus 3% in the radiotherapy-alone arm (p <0.02). Local control based on the findings at bronchoscopy was only 15% in the radiotherapy-alone arm with 85% of the patients still having persistent vital tumor. The benefit observed in this study was mainly derived from an increase of systemic control in the induction chemotherapy arm.
The fourth trial in this setting was a Nordic trial looking at induction therapy with cisplatin and etoposide followed by 56 Gy of a split-dose radiation therapy versus a “standard” radiation-alone arm with the same 56-Gy split-dose protocol.27 Three hundred and twenty-seven patients were randomized to the two treatment arms, and an increase in locoregional control was observed in the induction arm (4-year local failure-free survival rate of 7% vs. 3% in the radiotherapy-alone arm; p = 0.07). The difference showed a trend of improvement with the chemotherapy induction, but the benefit was not statistically significant. With overall 5-year survival rates being 3% in the induction arm and 1.4% in the radiotherapy-alone arm, no significant benefit for overall survival could be observed in this trial, either. It can only be speculated that the patient selection of this trial probably allowed a significant heterogeneity that may be responsible for the negative finding in this study.
Taken together the results of all four trials, induction chemotherapy prior to definitive radiotherapy resulted in a small but measurable benefit for overall and long-term survival in patients with stage III NSCLC. Critical commentaries should mention that in all four trials, the radiation protocols were far from being optimal concerning modern conformal radiation treatment planning standards. Also, the split-course radiotherapy application is biologically inferior and has been abandoned in the last years. Cumulative doses of 65 Gy are today accepted as standard treatment; therefore, only the French study fulfilled this rigid criterion. Cisplatinum-based chemotherapy application was still a problem at the time of performance of the first three trials. Modern antiemetic combinations represent a significant improvement for patients’ compliance to these intensive protocols. Radiotherapy treatment planning was not uniformly optimally based on CT scans and 3D planning, therefore leading to higher esophagitis rates within these studies.
A unique motif of all four trials was the cisplatinum-based induction chemotherapy combination. In light of the findings for adjuvant chemotherapy, it can be argued that two cycles of chemotherapy may have been suboptimal for the systemic efficacy on micrometastases in this setting; however, cisplatinum-based protocols are currently also the major choice for effective adjuvant chemotherapy in earlier disease stages.
When transferring the presented data to the stage IIIB NSCLC population, it can be concluded that cisplatin-based induction chemotherapy may generate a small but significantly long-term survival benefit based on the systemic efficacy of the combination chemotherapy and the high risk of systemic relapse in these patient subsets. Unfortunately, a further significant risk lies in the development of brain metastases in this patient group.28,29 Chemotherapy does not reduce the brain recurrence rate of these patient populations what can be derived from the large RTOG database.30 Other interventions (such as prophylactic cranial irradiation) should cover those competing risks if proven effective in the future.
Biologic Rationale of Concurrent Chemoradiotherapy in Lung Cancer Radiation therapy and cytotoxic chemotherapy theoretically can target different cellular pathways (e.g., DNA-damage, DNA-repair, apoptotic pathways, signal-transduction pathways), and thus may exert their major effects on different tumor cell populations. A concurrent application might lead to additive or even supraadditive effects on growing tumors.31 Concurrent chemotherapy to radiotherapy may prevent the development of radiotherapy-resistant tumor cell clones. Radiotherapy exerts its effect on the local and locoregional tumor. Chemotherapy not only exerts its effect locoregionally but on distant micrometastases (outside the brain) as well. By the effect of this so called spatial cooperation, the combination of both may lead to an increased overall effect of the simultaneous combination.32 These arguments have served as the major drivers of concurrent chemotherapy and radiotherapy protocols in locally advanced NSCLC. From other solid tumors, it is well-known that cisplatin alone already serves as a significant enhancer of radiation therapy effects. Within recent years, concurrent chemoradiotherapy protocols have gradually emerged as standard treatment approaches for different locally advanced solid tumors (e.g., esophageal cancer, cervical cancer, head and neck cancer).
Only gold members can continue reading. Log In or Register to continue