Lung cancer is the leading cause of cancer mortality in men and women in the United States, accounting for an estimated 161,840 deaths in 2008. Whereas lung cancer accounted for only 3% of all cancer deaths in women in 1950, in the year 2008 it accounted for an estimated 28% of cancer deaths. In 1990, the average annual mortality rate per 100,000 (standardized to the U.S. 2000 population) was 90.6 in men and 37.6 in women compared to 70.3 in men and 40.9 in women in 2004. Lung cancer incidence in men peaked in the 1980s and subsequently decreased after 1992 by 2.3% per year; mortality decreased 1.8% per year after having peaked around 1990. The age-adjusted lung cancer death rates in the United States surpassed those of breast cancer in white women in 1986 and in black women in 1990. It was estimated that in the year 2008, 30,550 more women will die of lung cancer (71,030) than of breast cancer (40,480).1
The incidence patterns, because of persistently poor survival rates, closely parallel the mortality rates. From 1992 to 2000, the average annual age-adjusted lung cancer incidence per 100,000 in men was 82.4, which was exceeded only by prostate cancer (180.6); the average annual lung cancer incidence in women was 49.4, which was second to that of breast cancer (132.5). In 2008, it was estimated that there were 215,020 new lung cancer cases diagnosed in the United States, and approximately 1.35 million cases were diagnosed world-wide with 1.18 million deaths in 2002.2
Lung cancer incidence and mortality patterns follow, after a latency interval of 20 or more years, the temporal patterns of cigarette smoking. In older men in the United States, lung cancer has displaced coronary heart disease as the leading cause of excess mortality among smokers. The risk of dying from lung cancer is associated with age of initiation and duration of cigarette smoking, and with the number and tar concentration of cigarettes smoked each day or as a regular pattern. The cumulative probability of lung cancer in the general population for individuals up to 74 years of age is 10% to 15% in those who smoke one or more packs of cigarettes per day. Exposure to other environmental and occupational respiratory carcinogens may be interactive with cigarette smoking and may influence trends of lung cancer incidence and mortality.3
DESCRIPTIVE EPIDEMIOLOGY
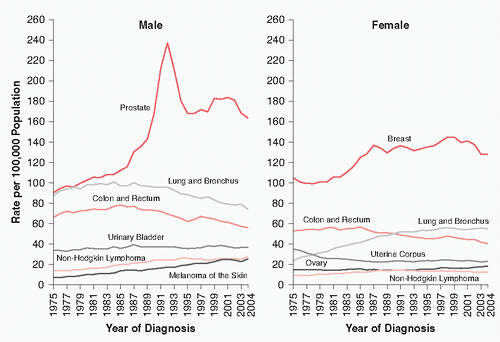
Age and Gender Whereas lung cancer incidence in men in the United States declined after peaking in the mid-1980s, the pattern in women differed significantly. In women, lung cancer incidence more than doubled between 1975 and 2000. Age-adjusted incidence in women increased on average by 4.1% per year between 1973 and 1990, but from 1990 to 2000, the average annual increase was only 0.2% (Fig. 1.1).
Among men and women, the rates declined in the past 10 years particularly among those younger than the age of 60 but continued to increase among those older than the age of 70. Only 5% to 10% of lung cancer cases are diagnosed in individuals younger than 50 years of age. Epidemiologic studies of lung cancer in young adults emphasize the predominance of adenocarcinomas and the importance of a positive family history. The current smoking prevalence and magnitude of estimates of relative risk (RR) caused by the average intensity and duration of smoking in women in the United States appear to be converging on the patterns in similarly exposed and aged men. Among whites, the male to female age-standardized lung cancer incidence ratio of rates is about 1:6, or 60% higher in men.4,5
Compared with women, men generally began smoking cigarettes at an earlier age, smoked more cigarettes per day and for a longer duration, inhaled more deeply, and consumed cigarettes with higher tar content. With increasing prevalence and duration of tobacco smoking in women after World War II, lung cancer mortality increased substantially in North America and Western Europe.
Several case-control studies have suggested that female smokers have a higher RR of lung cancer than male smokers, after adjusting for age and average daily intensity of smoking exposure.6,7,8 The case-control design and the method of estimation of odds ratios in women may have been susceptible to recall bias, underreporting of amount smoked by the cases, and differences in baseline confounding risk factors for lung cancer between male and female nonsmoking controls (e.g., occupational risk factors, nutritional risk factors, unmeasured exposure to environmental tobacco smoke, history of non-neoplastic lung diseases, etc.). Prospective studies are required to derive unconfounded incidence measures of absolute or attributable risk that may be compared in smoking and nonsmoking men and women. In an analysis of former and current smokers in the Nurses’ Health Study of women and the Health Professionals Follow-up Study in men, Bain et al.9 reported that the hazard ratio in women ever smokers compared with men was 1.11 (95% confidence interval, 0.95 to 1.31). The analytic model controlled for the number of cigarettes smoked per day, age at starting smoking, and time since stopping smoking. Freedman et al.10 compared the age-standardized incidence rates of lung cancer in men and women participating in the National Institutes of Health American Association of Retired Persons (AARP) cohort. In current smokers, in a model adjusted for lifetime smoking exposure, the hazard ratio was 0.9 (95% confidence interval, 0.8 to 1.0) for women compared with men. Both studies concluded that women were not more susceptible than men to the carcinogenic effects of cigarette smoking. Future studies should continue to monitor lung cancer incidence in women and men who have never smoked.
FIGURE 1.1 Annual age-adjusted cancer incidence rates for selected cancers by sex, United States, 1975 to 2004. Rates are age-adjusted to the 2000 U.S. standard population and adjusted for delays in reporting. Source: Surveillance, Epidemiology, and End Results (SEER) Program (http://www.seer.cancer.gov). Delay-Adjust Incidence database: Statistical Research and Applications Branch, released April 2007, based on the November 2006 SEER data submission. (From Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin 2008;58:71-96.)
Race and Ethnicity In the United States, the risk of lung cancer in black men has been about 50% higher than that in white men in the past 10 to 15 years, but the annual rate of decline after 1990 in black men (-2.5%) was about equal to that in white men (-2.3%) (Table 1.1). Among black men, lung cancer mortality was the second leading cause of death, ranking below coronary heart disease. The excess mortality from lung cancer among black men, compared with white men, was greatest for the age interval of 35 to 64 years. Cohorts of white men born before 1900 had higher (50%) age-specific rates than black men; however, this pattern reversed after 1915.
In the United States from 1975 to 1990, the age-adjusted lung cancer incidence in black women was 10% to 20% higher than that in white women; in the past 10 years, the average annual rate in black women (39.3 per 100,000) was slightly less than that in white women (40.9 per 100,000). After 1990, the incidence rates have continued to increase at an average annual rate of 0.7% to 0.8% for black and white women.
The Surveillance, Epidemiology, and End Results (SEER) program of the National Cancer Institute enables a comparison of risks among various racial and ethnic groups in the United States (Table 1.2). The lowest age-adjusted lung cancer incidence rates in men and women, 50% to 70% of the rates among non-Hispanic whites, were registered for Native Americans, Hispanics, and Asian-Pacific Islanders; the highest rates were reported in blacks, native Hawaiians, and non-Hispanic whites. The ratio of male to female incidence rates reflected elevated risks in men that were 2.5 to 3.5 times the rates in women from the various racial and ethnic groups. Although the age-adjusted lung cancer incidence rates varied substantially by ethnicity, the percentage of all cancer deaths attributed to lung cancer in men and women combined was as high in Native Americans (27.7%) as in African Americans (26.1%). Lung cancer is the leading cause of cancer mortality among Hispanic men and the second leading cause among Hispanic women.
TABLE 1.1 Age-Adjusted (1970 U.S. Standard) Lung Cancer Incidence per 100,000 in SEER Registry Areas by Race and Gender
*Per 100,000 population, age-adjusted to the 2000 U.S. standard population.
† Data based on Contract Health Service Delivery Areas (CHSDA), 624 counties comprising 54% of the U.S. American Indian/Alaska Native population; for more information, please see Espey DK, Wu XC, Swan J, et al. Annual report to the nation on the status of cancer, 1975-2004, featuring cancer in American Indians and Alaska natives. Cancer 2007 Nov 15;110(10):2119-2152.
‡ Persons of Hispanic/Latino origin may be of any race.
§ Incidence data unavailable from the Alaska Native Registry and Kentucky.
¶ Mortality data unavailable from Minnesota, New Hampshire, and North Dakota.
Adapted from Ries LAG, Melbert D, Krapcho M, et al., eds. SEER Cancer Statistics Review, 1975-2004, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2004/, based on November 2006 SEER data submission, posted to the SEER Web site, 2007.
It is generally assumed that the differences in rates of lung cancer can be partially explained by different lifetime patterns of cigarette smoking. Compared with non-Hispanic white men, a higher percentage of non-Hispanic blacks were current smokers, smoked cigarettes with greater yield of tar and nicotine, and preferred to smoke mentholated cigarettes, which may stimulate deeper inhalation of cigarette smoke. However, in surveys of current smokers, black men were reported to smoke fewer cigarettes per day than white men. Molecular and biochemical studies, when controlling for differences in smoking habits, described higher serum cotinine levels and 4-aminobiphenyl-hemoglobin adduct levels in black smokers when compared with white smokers, suggesting that there may also be differences in susceptibility between blacks and whites as expressed in the metabolism of tobacco smoke.11,12,13,14
Socioeconomic Status Various studies have reported an inverse association between lung cancer mortality and socioeco-nomic status (Table 1.3). A twofold gradient in mortality was observed between low and high social class, as measured by occupation, income, or education. Smoking patterns accounted for part of the differential risk by social class, with smoking prevalence increased among blue-collar workers and among those with lower levels of education. Socioeconomic status may also serve as a surrogate measure for other risk factors such as occupation, diet, and ambient air pollutants, and may influence the quality, access, and utilization of healthcare services.15,16
International Patterns Global lung cancer incidence is increasing at a rate of 0.5% per year, and as a consequence, lung cancer is the leading cause of cancer incidence and mortality in European countries, accounting for about 21% of all cancer cases in men.17,18,19,20 In less industrialized, developing countries, the proportion of all cancer deaths attributed to lung cancer is about 15%. In most parts of the world, rates were higher in urban than in rural areas and two to six times higher in men than in women. The areas with the highest incidence and mortality were in Eastern Europe, North America, Australia and New Zealand, and South America. The rates in China, Japan, and Southeast Asia were moderately high, whereas the lowest rates were observed in southern Asia, and in India and Pakistan, as well as in most countries in sub-Saharan Africa. Worldwide, in the year 2000, it was estimated that 47% to 52% of men and 10% to 12% of women smoked tobacco. In the United States, 25% of non-Hispanic white men and 23% of non-Hispanic white women were smoking tobacco. The prevalence of smoking men and women, the types of cigarettes and amounts smoked, ages at initiation and duration of smoking exposure, and proportions of heavy smokers in the population, were important determinants of geocultural variations in lung cancer incidence. Recent trends in lung cancer mortality in men exhibited declining rates in all European countries except in France, Greece, Portugal, and Spain. Cigarette smoking in China has followed a pattern similar to that among adults in the United States although the significant pattern of increase, particularly among men, occurred 40 years later. Of the Chinese deaths attributed to tobacco, 15% were due to lung cancer and 45% to chronic obstructive lung disease. The relatively elevated rates of adenocarcinoma of the lung among Chinese women in China and Singapore were attributed to exposures to smoking tobacco and to environmental pollutants other than smoking tobacco (e.g., fossil fuel combustion products and cooking oils in the home).21,22
TABLE 1.3 Lung Cancer Death Rates* by Educational Attainment, Race, and Sex, United States, 2001
Male
Female
African American
Non-Hispanic White
Absolute Difference
African American
Non-Hispanic White
Absolute Difference
≤12 years of education
73.23
60.99
12.24
30.82
37.06
-6.24
>2 years of education
25.78
18.13
7.65
17.92
14.20
3.72
RR (95% CI)
2.84 (2.69-3.00)
3.36 (3.30-3.43)
1.72 (1.61-1.84)
2.6 (2.53-2.67)
Absolute Difference
47.45
42.86
12.90
22.86
*Rates are for individuals aged 25-64 years at death, per 100,000, and age-adjusted to the 2000 U.S. standard population.
CI, confidence interval; RR, relative risk.
Adapted from Albano JD, Ward E, Jemal A, et al. Cancer mortality in the United States by education level and race. J Natl Cancer Inst 2007;99:1384-1394.
LIFESTYLE AND ENVIRONMENTAL RISK FACTORS
Tobacco The causal relationship between tobacco smoking and lung cancer was established by epidemiologic studies conducted in the 1950s and 1960s. The complexity of tobacco smoke, with over 3000 different chemicals, has made it difficult to identify the contribution of more than 50 putative carcinogenic agents. The carcinogens in tobacco smoke include the polynuclear aromatic hydrocarbons (PAHs), N-nitrosamines, aromatic amines, other organic (e.g., benzene, acrylonitrile) and inorganic (e.g., arsenic, acetaldehyde) compounds, and polonium-210. The composition of the smoke depends on the ambient conditions of smoking, the blend of tobacco leaf, filtration, additives, and paper wrapping. Tobacco smoke produced by the tobaccos in pipes and cigars is both harsher and more alkaline than that produced by cigarettes. Most of the compounds in tobacco are produced in an oxygendeficient, hydrogen-rich environment, arising from pyrolysis and distillation, in the region immediately behind the burning tip of the cigarette. The nicotine concentration is addictive and toxic but not carcinogenic.23,24
As mainstream cigarette smoke emerges from the cigarette, it has approximately 109 to 1010 particles per mL. The aerodynamic diameters of the particles, ranging in size from 0.1 to 1.0 μm, determine the sites of deposition in the airways and alveolar regions of the lung. The fraction of smoke retained varies markedly with the pattern of inhalation. The chemical analysis of tobacco smoke is separated into particulate or “tar,” and gaseous phases. Filter tips of cellulose acetate remove volatile nitrosamines and phenols selectively. The neutral fraction of the particulate phase contains potentially important tumor initiators such as the PAHs.25
In 1964, the first surgeon general’s report on smoking summarized existing evidence and declared cigarette smoking to be the major cause of lung cancer among American men.26 In the ensuing 30 years, epidemiologic studies have established that there were increasing risks in women and underscored the relationships with onset, duration, intensity, and cessation of smoking. Prospective studies demonstrated a rising trend in lung cancer death rates with increasing average amounts smoked per day in current smokers. The initial emphasis of epidemiologic studies of lung cancer and smoking was on men who, in almost all countries, began smoking earlier, consumed greater quantities of tobacco, and exhibited higher RRs than women.27,28,29
In the past 20 years, the prevalence of cigarette smoking in many countries, including the United States, has increased significantly among women; concomitantly, changes in smoking practices have been accompanied by increasing relative and attributable risks for lung cancer.30,31,32 In a follow-up study of approximately 600,000 women conducted in 1980s by the American Cancer Society, the RR of dying of lung cancer in current smokers was 12.7; for those who smoked 30 or more cigarettes per day, the RR was increased 22.3 times compared with the never-smoker. In 1985, cigarette smoking accounted for an estimated 82% of lung cancer deaths, or 31,600 deaths.33 The International Agency for Research on Cancer (IARC) estimated that the smoking-attributable fraction of lung cancer deaths occurring in the United States and in England and Wales was 92% in men and 78% in women.25 In 2001, the U.S. Health Interview Survey estimated that 46.2 million adults were current smokers and that 44.7 million adults were former smokers. Current smoking prevalence was highest among persons aged 18 to 24 years (26.9%), and among those aged 25 to 44 years (25.8%), and lowest among those aged older than 65 years (10.1%). From 2000 to 2001, current smoking prevalence, for the first time, was similar in non-Hispanic white (25.4%) and black (27.7%) men; in contrast, the prevalence in non-Hispanic black women (17.9%) was less than that in non-Hispanic white women (22.8%).32
Lower tar content and the use of filters are factors that may result in reduced lung cancer risks in those who smoke. In the earlier American Cancer Society (ACS) Twenty-five-State Study, men who smoked low-tar (<22 mg) cigarettes experienced 20% lower risk of dying of lung cancer when compared with men who continued to smoke high-tar cigarettes. The excess lung cancer risk for current smokers was directly proportional to the estimated milligrams of tar consumed daily. In the more recent ACS Fifty-State Study, Garfinkel and Stellman concluded that doubling the cigarette tar yield would result in a 40% increase in the RR of dying of lung cancer, independently of the amount smoked or depth of inhalation. The Federal Trade Commission estimated that the current average salesweighted tar content of cigarettes manufactured in the United States was about 12 to 13 mg of tar per cigarette, compared with nearly 40 mg in the early 1950s. Lifelong filter cigarette smokers have experienced 20% to 40% lower risk of lung cancer than lifelong nonfilter smokers, after adjusting for differences in the amount smoked. Presumably, larger reductions in risk have not been observed because of alternations in smoking behavior in response to low-nicotine yield of manufactured cigarettes. Namely, it has been shown that in maintaining addiction, the smoker will inhale larger volumes of mainstream smoke and at more frequent intervals.34,35,36,37
Although these studies suggested that switching to filtered or low-tar cigarettes may modestly reduce the risk of lung cancer, the more significant reduction in risk would be derived from cessation of smoking. Whereas approximately 25% of smoking adults in the United States continue to smoke, an additional 40% to 50% have become former smokers. The RR of lung cancer among ex-smokers decreases significantly after 5 years of smoking cessation. In the initial 1 to 4 years after quitting smoking, however, the RR of lung cancer among ex-smokers may appear to be higher than among current smokers, presumably because a proportion of individuals may have stopped smoking because of illness or premonitory symptoms of lung cancer.38,39
It has been suggested that the risk of lung cancer in former smokers will approximate but never equal that of lifelong nonsmokers. The baseline risk of lung cancer in lifelong nonsmokers increases in relation to age raised to the fourth or fifth power. In the British Physicians Study, Doll and Peto38 showed that the incidence of lung cancer in cigarette smokers increased approximately in proportion to the fourth power of duration of smoking, and was multiplicative with the previously described exponential increase with age among never-smokers. The percentage reduction in risk after quitting depended on the prior duration and average amount smoked each day, being more readily demonstrable among lighter smokers and smokers of lesser duration or those who quit at a younger age. Lung cancer results from a multistep process in which persistent genetic lesions accumulate at specific chromosomal loci. Most current or former smokers, in contrast to never-smokers, exhibit loss of heterozygosity at multiple allelic sites (e.g., 3p14, 9p21, p16, p53) in both normal and metaplastic or dysplastic bronchial epithelium.40,41
Pipe and cigar smoking have been linked to lung cancer, particularly squamous cell and small cell carcinomas, but the estimated RRs, compared with people who never smoked, who are assigned an RR of 1.0, were considerably lower than the risks reported among cigarette smokers; the risks among exclusively pipe or cigar smokers in the United States or Europe have been estimated to range from 2.0 to 9.0. In countries such as Sweden, Switzerland, and Holland, where pipe or cigar smoking was nearly as common as cigarette smoking, the RRs of lung cancer, when controlling for cumulative exposure levels, were equally high for all forms of smoked tobacco. Differences in the manner in which pipes and cigars were smoked in different countries, (i.e., depth of inhalation or average daily or cumulative amount smoked) may provide an explanation for differences in the estimated risks. Cigars are products made of tobacco, wrapped in tobacco leaves rather than in paper. Cigars smoked in Europe weigh 2 to 8 g and are similar to American “small cigars.” Cigarillos are smaller than cigars weighing 1.5 to 3 g and are described as “little cigars” in the United States. Risks of lung cancer also varied with the type of tobacco used. Dark tobaccos were associated with greater risk of lung cancer than light tobaccos, and with formation of higher levels of 4-aminobiphenyl-hemoglobin adducts.42,43,44,45
Environmental Tobacco Smoke Environmental tobacco smoke (ETS) is comprised of sidestream smoke (about 80% released from burning tobacco in between puffs), and from the exhaled smoke (about 20% of the smoke). The smoke that the smoker inhales is known as mainstream smoke. Other minor contributors to ETS include the smoke that escapes during puffing from the burning cone, and gaseous components that diffuse through the cigarette paper. These components are diluted by the ambient air and when inhaled, in particular by nonsmokers, are referred to as “passive” or “involuntary” smoking. ETS contains various toxic agents, including mutagens and carcinogens, which, for some chemicals (e.g., nitrosamines, 4-aminobiphenyl, benzo[a]pyrene), have been measured at higher concentrations than in mainstream smoke. Estimates of ETS exposure, based on serum or urinary measurements of cotinine, the metabolite of nicotine, suggest that involuntary smokers absorb about 0.5% to 1% of the nicotine that active smokers absorb, or smoke the equivalent of about one-half cigarette a day. Studies of 4-aminobiphenyl-hemoglobin adduct levels indicate that passive smokers have approximately 14% of the concentration of active smokers.46
Many scientific consensus committees have concluded that exposure to ETS causes lung cancer in humans. Table 1.4 lists the RRs of lung cancer among nonsmoking women based on a review of epidemiologic studies in various countries, which have evaluated dose-response trends.47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63 and 64 The risks increased with amounts smoked by husbands, with about 30% to 150% increases in RR experienced in general among those women most heavily exposed. A weighted analysis of 37 published epidemiological studies resulted in the conclusion that there was an elevated risk of 24% (95% confidence interval [CI], 13% to 36%) among nonsmoking wives of smoking husbands, when compared with nonsmoking wives of nonsmoking husbands. Workplace exposures to ETS are measured with less precision than spousal exposures; however, some studies have suggested that there is a dose-response relationship when combining workplace and spousal sources of ETS. It has been suggested that when using biological markers of nicotine exposure in studies of ETS and lung cancer, about 5% of female respondents, who were in fact smokers, may have reported that they were nonsmokers. Correcting for this bias, however, would result in an adjusted RR in nonsmoking women who were living with smokers of about 1.15 to 1.20. The report of the National Research Council concluded that about 20% of lung cancers occurring in nonsmoking women and men, or 3000 cases per year, may be attributable to exposure to ETS; in the context of lung cancer cases diagnosed each year in smokers and nonsmokers, 2% to 3% may be attributable to ETS.65,66
TABLE 1.4 Relative Risk of Lung Cancer among Nonsmoking Women According to Level of Husband’s Smoking
* Definitions of heavy smokers varied by study, but typically included those who smoked 20 or more cigarettes per day.
Air Pollution Pollutants in the urban air other than from tobacco have been investigated as potential causal agents in the epidemic rise of lung cancer in industrialized nations. The products of fossil fuel combustion, principally polycyclic hydrocarbons, have been of particular concern. Other sources of ambient air pollution have been motor vehicle and diesel engine exhausts, power plants, and industrial and residential emissions. The ratio of urban to rural age-adjusted lung cancer mortality rates in many industrialized nations have varied between 1.1 and 2.0. It has been suggested that the net attributable risk effect of protracted exposure to urban air pollutants in men with average smoking habits would be 10 cases of lung cancer per 100,000 per year. In most countries, however, a major fraction (i.e., 80% or greater) would be attributable to cigarette smoking, and the independent association with urban residence, or the “urban factor,” could not be assessed without controlling for the confounding effect of differences in smoking practices, or exposures to environmental tobacco smoke, between urban and rural residents. In addition, the urban factor has yet to be defined, but is undoubtedly a complex mixture of interacting chemical compounds and elements that vary by geographic area and over time. Exposure to combustion-source ambient air pollution has been associated with declining pulmonary function, increased rates of hospitalization for respiratory illnesses, and increased rates of cardiopulmonary diseases mortality.67,68,69
Only gold members can continue reading. Log In or Register to continue