Chapter 141
Splanchnic Artery Aneurysms
Ryan O. Lakin, Vikram S. Kashyap
Based on a chapter in the seventh edition by Caron B. Rockman and Thomas S. Maldonado
Aneurysms of the splanchnic arteries are a rare entity, but they mandate clinical awareness due to their lethal nature. First described in European literature more than 200 years ago,1 premodern surgical management of splanchnic artery aneurysms consisted mostly of emergent intervention, with many cases identified postmortem after rupture. Very few case reports existed before the De Bakey et al publication in 1953, which described the first successful treatment of a superior mesenteric artery (SMA) aneurysm.2 The first large case series appeared in the 1980s because modern imaging techniques allowed for preemptive discovery and management of these often asymptomatic aneurysms. A recent review cited close to 3000 reported cases in the literature.3 Marked changes in treatment modalities occurred over the past decade with the advent of endovascular therapies. Additionally, modern imaging techniques allowed surveillance to be a safe option in selected cases, akin to aneurysmal disease of the abdominal aorta. However, aneurysms of the visceral vasculature remain potentially lethal entities with a poorly understood natural history. Consensus is slowly gathering in the vascular literature regarding the standard of care. In this chapter, we consolidate observations from both early and recent case series and examine treatment guidelines for splanchnic artery aneurysms.
Incidence and Etiology
Splanchnic (or visceral) artery aneurysms are defined as those affecting the celiac artery, SMA, inferior mesenteric artery (IMA), and any aneurysm affecting the branches of these arteries. Importantly, aortic and renal artery aneurysms are excluded in this categorization, although 95% of all intra-abdominal aneurysms occur along the course of the aortoiliac and renal vasculature.4 Nearly one third of patients with a splanchnic artery aneurysm will have an associated aortic, renal, iliac, lower extremity, or cerebral artery aneurysm. Splanchnic aneurysm incidence in the general adult population is estimated to range from 0.1% to 2%,5–9 which increases to 10% in the elderly population based on autopsy review.10 Splenic artery aneurysms (SAAs) encompass the majority (60%), followed by hepatic artery aneurysms (HAAs; 20%), superior mesenteric artery aneurysms (SMAAs; 5.5%), celiac artery aneurysms (CAAs; 4%), gastric artery aneurysms (GAAs; 4%), jejunal, ileal, and colic arteries aneurysms (3%), pancreaticoduodenal artery aneurysms (PDAAs; 2%), gastroduodenal artery aneurysms (GDAAs; 1.5%), and inferior mesenteric artery aneurysms (IMAAs; <1%) (Fig. 141-1).11–13
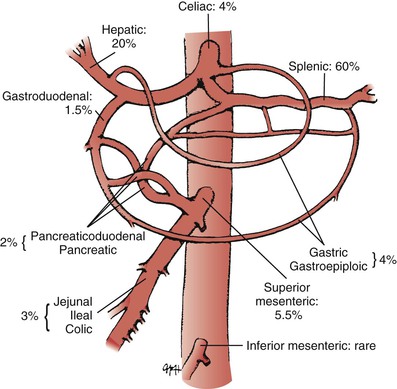
Figure 141-1 Relative incidence of aneurysms affecting the arteries of the splanchnic circulation as reported in the literature.
Traditionally, aneurysms are defined as dilation or enlargement of an artery to more than 1.5 to 2 times its normal diameter.14 Saccular aneurysms are focal and may be eccentric, whereas fusiform aneurysms are elongated and usually concentric.15 These two distinctions are mentioned largely in pathology and radiology reports, and have no established significance pertaining to differences in etiology or rupture risk. A recent study has shown that wall stress for saccular descending thoracic aortic aneurysms is greater than that for fusiform aneurysms, indicating that geometric factors, such as aneurysm shape, influence wall stress.16 These results suggest that saccular descending thoracic aortic aneurysms may be more prone to rupture than fusiform aneurysms of similar diameter; however, this principle has not been studied in splanchnic vasculature. Saccular and fusiform morphology may ultimately affect treatment options when endovascular therapies are applied.
The etiology of splanchnic artery aneurysms differs for true aneurysms versus pseudoaneurysms. Causes of true splanchnic aneurysms include atherosclerosis, medial degeneration, collagen vascular diseases, and fibromuscular dysplasia.17 Other factors such as multiparity, portal hypertension, and posttransplant status have been associated specifically with SAA formation.3,18,19 Splanchnic pseudoaneurysms result from infectious or inflammatory conditions, vasculitis, surgery or other iatrogenic intervention, and trauma.17,20,21 The rising number of percutaneous and laparoscopic procedures has contributed to a greater number of reported hepatic pseudoaneurysms.12,22–24 Importantly, evidence suggests that pseudoaneurysms display relatively rapid growth rates soon after the initial insult, such that treatment strategies should focus on early intervention, regardless of size.25
Special Considerations for Associated Conditions
Rare medical conditions, such as von Recklinghausen’s disease, Ehlers-Danlos syndrome, and periarteritis nodosa (PAN) have been implicated in the development of splanchnic aneurysms. Reported case series have demonstrated the association of multiple splanchnic aneurysms with systemic arteritis, endocarditis with septic emboli, connective tissue disorders, and even excessive acetaminophen use.26
Von Recklinghausen’s Disease
Vasculopathy associated with the syndrome of Von Recklinghausen’s neurofibromatosis, first described by Reubi in 1945, is a clinically significant phenomenon.27 Manifestations include renovascular hypertension, occlusive cerebrovascular disease, visceral ischemia, and aneurysm formation.28–30 Patients may present with several aneurysms affecting multiple vascular beds, which creates obvious therapeutic challenges.31,32 Vascular lesions associated with von Recklinghausen’s disease are particularly difficult to treat because of the vessel wall frailty that develops from this disease process.
Ehlers-Danlos’ Syndrome
Much like von Recklinghausen’s disease, the inherited connective tissue disorder Ehlers-Danlos’ syndrome type IV predisposes affected patients to aneurysm formation in splanchnic and other arteries due to loss of vessel wall integrity.4 On rare occasions, patients may present with spontaneous rupture at relatively young ages.33–35 Any evaluation should be performed with noninvasive means, such as ultrasound, computed tomography (CT), or magnetic resonance angiography. Open surgical treatment can be technically futile with collagen levels at less than 10% of normal in some patients with Ehlers-Danlos.36,37 Elective surgery should be avoided, and endovascular therapy can be considered as an alternative for intervention.
Periarteritis Nodosa
Unlike the aforementioned connective tissue disorders, PAN is considered to be a type of necrotizing vasculitis.38 It often involves small- and medium-sized visceral arteries, and may result in multifocal aneurysmal formation and end-organ damage.39 This condition can also affect relatively younger patients, and spontaneous rupture is reported in the literature.40 Interestingly, aneurysms associated with PAN show regression when treated with pharmacologic immunosuppression or cytotoxic therapies.41–43
Rupture Risk
The rarity and insidious nature of splanchnic artery aneurysms creates an extreme challenge in both emergency diagnosis and treatment. Before modern imaging techniques were readily available, many splanchnic artery aneurysms were discovered at autopsy, with rupture being the cause of death. Presumably in these cases, aneurysms had silent progression in size over years until rupture. It has been reported that nearly 22% of all patients present as clinical emergencies, including 8.5% whose splanchnic aneurysms result in death.11 Aneurysm rupture in the setting of circulatory collapse is a devastating clinical scenario, with perioperative mortality rates reported from 20% to 70% depending on location, etiology, and other contributing factors.25,44–48
Splenic Artery Aneurysms
SAAs have a relatively low rupture rate of less than 2% in cases not associated with pregnancy.49 Mortality rates in these cases range from 10% to 20%. The phenomenon of “double rupture” may manifest in 25% of these cases, which occurs after initial tamponade of splenic artery hemorrhage into the lesser sac, which may delay free rupture into the retroperitoneum by as much as 4 days.50,51 Special attention must be considered for SAAs in pregnant women. Maternal mortality approaches 75% in the setting of ruptured SAAs, with a concomitant fetal mortality of 95%.52,53 Although the true prevalence of SAA in pregnancy or women of childbearing age is estimated to be less than 0.1% in one series,54 it is thought that more than 50% of them rupture during pregnancy, with two thirds of these rupturing in the third trimester.55,56 The association between higher SAA incidence and/or rupture and portal hypertension has also been documented, especially in patients who have undergone orthotopic liver transplantation.19
Other Splanchnic Aneurysms
The precise rates of rupture for less prevalent splanchnic artery aneurysms may never be definitively established, nor have the risk factors associated with their rupture been thoroughly elucidated. Reported rates of rupture for HAAs are 60% to 80%, 38% for SMAAs, 7% for CAAs, 68% for PDAAs, 56% for GDAAs, and 90% for gastroepiploic artery aneurysms.11,47,57,58 These rates are based largely on published reports and review series, which are limited to actual cases reported. The increased use of modern imaging modalities, such as CT and magnetic resonance imaging (MRI), that discover incidental disease processes may ultimately offer a refined prevalence of these infrequently encountered splanchnic artery aneurysms.
General Treatment Principles
Advances in endovascular therapies have caused a paradigm shift in the management of splanchnic artery aneurysms. Several large retrospective series have proven minimally invasive management with either coil or glue embolization to be a safe and durable option.7,17,25,45,59–63 However, these aneurysms can also be managed with open surgery, laparoscopic surgery, or by minimally invasive endovascular techniques.57 Some cases are best managed with the incorporation of two modalities in a staged procedure approach.64,65 The use of minimally invasive endovascular techniques affords several options, including the use of coils, covered stents, glue, thrombin, or a combination of these. There have been recent case reports describing the successful use of ethyl chloride injection, CT-guided direct percutaneous injection of thrombin, and even robot-assisted procedures.66–70 A recent review of 27 published case series of splanchnic artery aneurysm repair over the last 20 years concluded that there is no consensus about precise indications or the best type of surgical treatment.71 Expert opinion indicates that this is guided by both patient and aneurysm characteristics. Age, gender, and presence of comorbidities must also be taken into account. The size of the aneurysm, anatomic location, and collateral circulation may dictate the surgical option to be chosen.
Elective Repair
The elective treatment of splanchnic artery aneurysms allows for complete evaluation and imaging with ultrasound, CT, MRI, or a combination of these.72 Conventional arteriography may be used for diagnosis in selected cases, but is usually reserved for percutaneous intervention of the aneurysm. In addition, arteriography may also be useful as a preoperative imaging modality to assess adequate collateralization to the end organ. A thorough patient evaluation should address any history of trauma, pancreatitis, or any other infectious and/or inflammatory process to ascertain etiology and risk of rupture. Past surgical intervention or hepatobiliary instrumentation, current pregnancy status, history of pregnancies, and risk factors associated with atherosclerosis are also pertinent. If available, previous imaging should be reviewed to assess any growth of the aneurysm. A cardiac workup and risk stratification should be obtained for selective patients.73 Patients undergoing SAA embolization or ligation may be at risk for splenic loss and should receive Pneumococcal vaccine.74
Emergent Repair
Ruptured splanchnic artery aneurysms represent a true surgical emergency, and patients should be expeditiously transferred to the operating room for exploratory laparotomy in the setting of hemodynamic collapse. Often, the preoperative diagnosis is a ruptured abdominal aortic aneurysm, and only exploration leads to the identification of the actual ruptured artery. Ligation of a splanchnic aneurysm can be performed with or without vascular reconstruction. Patients presenting with ruptured SAA are most often treated with concomitant splenectomy. Given the extensive collateralization of the viscera, vascular reconstruction is rarely needed in emergent treatment of proximal HAAs, PDAs, and GAAs.46,47 When mesenteric arterial aneurysms are ligated, any small bowel affected by ischemia may require resection. Arterial reconstruction may be necessary for ruptured SMAAs and CAAs. Endovascular management of ruptured splanchnic artery aneurysms has been reported as a feasible option, but should only be used in selective stable cases.75,76
Observation
Most large case series of splanchnic artery aneurysm management have included an observation cohort with encouraging results.* The majority of observational cases involve the splenic artery. General guidelines state that SAAs less than 2 cm in size that are asymptomatic and show little to no growth can be safely observed and monitored with serial imaging. Women who are either pregnant or of childbearing age should have any SAA treated, regardless of size.80 There is no firm evidence to show that aneurysm calcification protects against growth or rupture, but calcified SAAs may be associated with smaller size at initial diagnosis.77 Most series advocate for all pseudoaneurysms to be treated, irrespective of size or location due to their increased growth rate and propensity to rupture.23,81 There is also evidence to support treating all SMAAs due to their high rupture rate and associated mortality (Fig. 141-2).82
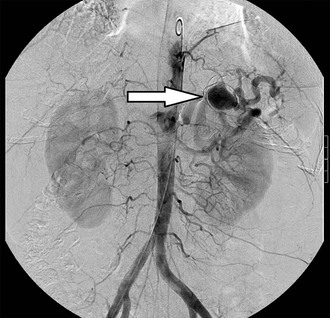
Figure 141-2 A 2.7-cm splenic artery aneurysm (arrow) is visualized during an abdominal angiogram. A calcified shell covers the aneurysm sac, with flow maintained to the end organ.
Surgical and Endovascular Techniques
Open Repair
Treatment of splanchnic artery aneurysms with open surgery has been established as a safe and durable standard.79,83 Open surgical repair may include aneurysmectomy and bypass grafting, aneurysmectomy and end-to-end anastomosis, aneurysmorrhaphy, and/or ligation. An open surgical approach allows for direct visualization of end organs, concomitant diseases processes (e.g., pancreatic pseudocysts or abscesses), and is useful for determining the need for arterial reconstruction if intestinal viability is compromised. In addition to its proven durability, the use of an open surgical approach mitigates the need for closer follow-up and serial imaging required after endovascular therapies. Expeditious ligation of both the proximal and distal branches is generally performed without the need for reconstruction in the case of frank rupture and hemodynamic collapse, and often during elective cases if adequate collateralization to end organs is present.44 The spleen has a rich blood supply from the short gastric arteries and pancreaticoduodenal arcade, which usually allow the splenic artery to be sacrificed without major consequence. The celiac axis and common hepatic artery can also be ligated if sufficient collateralization exists from the gastroduodenal and pancreaticoduodenal arteries, and if the portal vein is patent. Even the proximal SMA has been ligated in emergency cases. Most often, however, aneurysms of these visceral branches require concomitant ligation and revascularization. Vein grafts should be used preferentially in cases of suspected infection or bowel ischemia.
All open procedures should be performed under general anesthesia. The use of an epidural catheter may assist in postoperative pain control. Arterial ligation is the procedure of choice in the setting of free rupture. The surgeon must be diligent in achieving both inflow and outflow ligation. Although laparoscopic treatment has shown to be an effective alternative in treating SAAs, its use seems to be best reserved for treating aneurysms located in the distal artery close to the splenic hilum.84–86 Laparoscopy has not been established as a treatment modality in ruptured cases, and is also relatively contraindicated in the pregnant female patient due to the associated risk of developing acidosis and hypercapnia.
Endovascular Therapy
The advent of minimally invasive endovascular therapies has influenced nearly all realms of vascular surgery and has certainly affected the management of splanchnic artery aneurysms in a profound manner. The immediate benefits associated with endovascular intervention include shorter hospital stay, local and/or conscious sedation use, decreases in cost, and faster recovery. Patients with comorbidities prohibitive to open surgical management, including intra-abdominal malignancy and previous surgery, can also benefit from minimally invasive techniques.87 Drawbacks to endovascular repair include the risk of access-related injury, contrast toxicity, end-organ embolization, and a relatively higher rate of failure compared with open surgery, and the need for prolonged postembolization imaging surveillance. Treatment by endovascular intervention can be achieved through several different modalities, including deployment of coils and glue, particle or gelfoam injection, placement of covered stents, flow-diverting stents, and injection of thrombin or ethyl alcohol.61 The treatment chosen is individualized to the clinical scenario, and optimal results can be achieved with knowledge of the endovascular armamentarium.
A recent publication from the Cleveland Clinic reported results of the endovascular treatment of 48 consecutive patients (mean age 58 years; 60% men) with 20 splanchnic artery aneurysms and 28 splanchnic artery pseudoaneurysms.25 The endovascular treatment of visceral artery aneurysms was technically successful in 98% of 48 procedures, consisting of 20 splenic arteries, 12 hepatic arteries, 1 SMA, 3 celiac axis, 2 pancreaticoduodenal arteries, 2 left gastric arteries, 7 gastroduodenal arteries, and 1 middle colic artery. Coil embolization was used for aneurysm exclusion in 96% of cases, and N-butyl-2-cyanoacrylate (glue) was used selectively in 19% of cases. The 30-day mortality was 8.3%, with all perioperative deaths occurring in patients who required urgent or emergent intervention because of hemodynamic instability. Complete exclusion of flow within the aneurysm sac occurred in 97% of interventions with follow-up imaging, with three (6%) patients developing postembolization syndrome after splenic artery embolization. A similar publication from the Mayo Clinic reported treatment results of 185 splanchnic artery aneurysms encountered over 10 years.61 Thirty-four percent of the aneurysms were located in the splenic artery, followed by 30% in the hepatic artery. Initial intervention was successful 98% of the time. Coiling was used alone in 75% of the cases, and in combination with at least one other technique in 11% of cases. Thirty-day, aneurysm-related mortality was low at 3.4%, and all deaths were due to bleeding.
Access via the right femoral or left brachial artery is preferred. All patients undergoing elective endovascular ablation should be systemically anticoagulated with heparin to achieve an activated clotting time of more than 250 seconds. Hemodynamically stable patients with rupture may receive small doses of heparin (2000-3000 U) after selective visceral cannulation. A 5F, 6F, or 7F long sheath is crucial to accommodate vascular devices. It is critical that the sheath be well placed into the proximal splenic or hepatic artery proximal to the aneurysm. Intravascular ultrasound can be used to augment the surgeon’s view of the aneurysm location via axial imaging.
Embolization
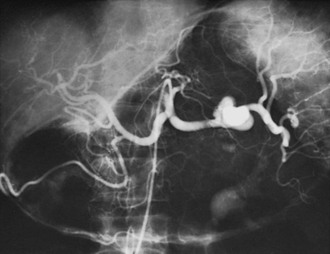
Ablation of splanchnic artery aneurysms through endovascular intervention can be accomplished with nitinol coils, cyanoacrylate glue, thrombin, and even ethyl alcohol.66,88–91 The rate of glue polymerization can be altered for precision targeting using ethiodized oil dilution. A ratio of 1 : 1 oil-to-glue is preferable to embolize a vessel with high rates of blood flow. Dilution ratios of 2 : 1 or 3 : 1 are ideal when the blood flow rates are slower or the catheter tip cannot be closely approximated to the desired site of polymerization. A 3F microcatheter is useful for interventions in the distal aspect of an arterial bed for selective deployment of embolization material.25 Both true and pseudoaneurysms of the splanchnic circulation can be managed with embolization. Endovascular exclusion to ablate both inflow and outflow can be achieved by placement of coils first distally to the sac and then proximally to the sac. For aneurysms supplied by terminal branches, the sac can be directly injected or coiled (Fig. 141-3).92


Covered Stents
In selected cases, a covered self-expanding stent may be placed to maintain flow within a vessel. This technique is often limited by relatively large and rigid delivery devices that are not ideal for navigating secondary and tertiary visceral branches. Covered stents also risk occluding flow into side branches of the target vessel. Covered and noncovered stents are, however, particularly useful when treating a hemodynamically significant dissection resulting from visceral vessel cannulation. Size discrepancies in the target vessel can lead to endoleaks and in-stent thrombosis. Oversizing of the endograft should be avoided. Target vessels presenting a size discrepancy between proximal and distal seal zones should be treated with a self-expanding model preferentially to a balloon-expandable model (Fig. 141-4).


Figure 141-4 A, Splenic artery aneurysm measuring 2 cm in size. B, Exclusion is achieved with a covered stent. Postdeployment imaging demonstrates that flow is maintained to the end organ.
Although limitations exist, covered stents are an alternative treatment modality in the endovascular management of splanchnic artery aneurysms, offering the key advantage over coil and glue ablation techniques of preserving prograde blood flow. Their use has been proven safe in several major visceral branches, with an excellent success rate and safety profile.93–97 Follow-up imaging is not limited by artifacts from radiopaque coils or glue, and this notable advantage of covered stent placement over embolization allows for accurate documentation and surveillance of aneurysm sac growth or shrinkage.98
Flow-Diverting Stents
Anatomic factors have placed limits on the application of traditional stent grafts for the treatment of splanchnic artery aneurysms. Flow-diverting stents (FDSs), sometimes referred to as multilayer stents, are specially designed to reduce flow velocity in the aneurysm sac while promoting thrombosis and maintaining flow within the main artery and any branch vessels. The FDSs were originally developed for the endovascular treatment of intracranial aneurysms. By 2010, this technology had been used to treat more than 2500 intracranial aneurysms.99 Initial case reports demonstrated FDS success in multiple peripheral and splanchnic vascular vessels.100–105 A prospective, multicenter study of FDS use in 19 splanchnic artery aneurysms recently reported encouraging results of freedom from rupture, patency of the stents and vessel branches, aneurysm thrombosis, sac shrinkage, and low morbidity and mortality.106
Specific Splanchnic Aneurysms
Splenic Artery Aneurysms
Epidemiology
SAAs have been established as the most common of the splanchnic artery aneurysms, accounting for nearly 60% of reported splanchnic aneurysms. Like any splanchnic artery aneurysm, their clinical significance is related to the potential for rupture. The most accurate calculated incidence in the general population is most often cited as 0.78%, which is based on a review of incidentally noted SAAs seen on nonselective angiography.107 One general autopsy study cited overall incidence to be 0.01%,108 with incidence increasing to 10.4% in an elderly population autopsy series.10 In contrast to other arterial aneurysms, SAAs disproportionately affect women at a ratio of 4 : 1 over men.44,56 Although incidence increases markedly in the elderly population, they occur at a younger age compared with other splanchnic aneurysms (Fig. 141-5).56,107
Most SAAs are close to 2 cm in diameter when initially noted. Reports of SAAs associated with symptoms and/or with rupture average closer to 3 cm at presentation.3,77,109 The majority of these aneurysms have saccular morphology and are located more commonly in the mid or distal splenic artery and its bifurcations.56,110 The rare phenomenon of so-called “giant” SAAs more than 10 cm in size has been encountered in the literature and seems to be found more often in men.111
Etiology
The underlying pathologic processes in the development of most SAAs are related to atherosclerosis, arterial fibrodysplasia, and arteritis.24,107 Associated risk factors include female gender, multiparity, and portal hypertension.19,56 Several reports have established association with multiparity and SAA development,3,109 but the precise interactions of hormonal influence, fibromuscular dysplasia, and wall stress are not yet fully understood.75,112 Some series have noted nearly 50% of women with more than six pregnancies have been diagnosed with an SAA.110,113 Another series noted that 80% of women with SAAs had an average of 4.5 pregnancies.109 Still, the utility of screening women for SAAs who are either pregnant or of childbearing age has been proven to be unwarranted in one recent study.54
The association between SAA and portal hypertension has been documented, especially in patients undergoing orthotopic liver transplantation.11 Evaluating patients with known portal hypertension or cirrhosis showed a likely SAA incidence ranging from 10% to 20%,114 with one study reporting an incidence as high as 50%.18 Notable etiologies of splenic artery pseudoaneurysm formation include blunt trauma, infection, and pancreatitis.23 Pseudoaneurysm formation associated with pancreatitis has been attributed to digestion of the splenic artery by pancreatic enzymes.115 Hemosuccus pancreaticus is a rare cause of upper chronic and intermittent gastrointestinal hemorrhage, usually due to the rupture of a visceral aneurysm into the main pancreatic duct. Splenic artery pseudoaneurysm formation associated with chronic pancreatitis represents the leading cause of this hemosuccus pancreatitis and is a challenging clinical scenario.116
Clinical Presentation
Before the introduction of modern imaging techniques and their abundant use in everyday practice, it was estimated that more than 10% of SAAs were ruptured at the time of diagnosis.56,113 Most current case series report that SAAs are incidental findings noted on imaging performed for unrelated symptoms. Incidental diagnosis can be presumptive many times based on circular calcified shadows or “signet rings” seen in the left upper quadrant of an abdominal roentgenogram.51 A relatively small percentage of patients will present with vague abdominal pain or even an abdominal bruit; however, most patients with otherwise asymptomatic SAAs will have benign physical examinations. The rare giant SAAs described in case reports may produce vague symptoms related to mass effect on the adjacent viscera, but there are also cases of asymptomatic patients with SAAs of more than 10 cm in size.65,117 Hemodynamic collapse secondary to rupture is most often accompanied by acute left-sided abdominal pain. The patient will typically present in extremis as a result of free intraperitoneal rupture and shock.108 On rare occasions, the initial rupture may be contained in the lesser sac and provide an optimal window of opportunity for noninvasive diagnosis and subsequent endovascular intervention. The clinician must be familiar with the “double rupture” phenomenon that occurs after initial tamponade of splenic artery hemorrhage into the lesser sac, which can prolong free rupture into the retroperitoneum by as long as 4 days.22,51,118 Pseudoaneurysms of the splenic artery may also rupture into adjacent structures, including the gastrointestinal tract, pancreatic duct, splenic vein, and can even form pancreatic pseudocysts.119–121
Mortality associated with ruptured SAAs ranges from 10% to 25%.3,51,110 Pregnancy is a significant contributing risk factor and may be associated with as many as half of all ruptures.55,56 Significant maternal and fetal mortality has been documented to be close to 70% for pregnant women and approximately 90% for the fetus.122 Rupture occurs almost exclusively in the third trimester; to date there have only been three reported cases of first trimester rupture in the literature.123 Portal hypertension is an additional significant risk factor, associated with nearly 20% of all SAA ruptures.109 A recent review of English and French literature found only 613 reported cases of splenic rupture without risk factors or previously diagnosed disease.124 The most common associated diseases in these patients were infectious in nature, followed by hematologic and nonhematologic neoplasms. Other associated conditions included amyloidosis, internal trauma such as cough or vomiting, and rheumatologic diseases. Colonoscopy was the procedure reported most frequently associated with rupture. Common medications associated with rupture included anticoagulants, thrombolytics, and recombinant granulocyte-colony stimulating factor.125
Treatment
All patients who present with a ruptured SAA should undergo immediate and definitive treatment. Additionally, any patient who has symptoms attributed to a nonruptured SAA should undergo intervention. Given the increased risk of rupture, patients who will undergo orthotopic liver transplantation or have portal hypertension are considered candidates for prophylactic SAA repair. Asymptomatic women who are pregnant or are of childbearing age should undergo treatment as well. Most advocate for the treatment of any splenic artery pseudoaneurysm, regardless of size or symptoms, due to their propensity to rupture. In the absence of the preceding scenarios, the threshold for intervention is based mainly on size of the aneurysm and/or rate of growth. Consensus in the literature has generally established the indications for treatment to include those aneurysms more than 2 cm in size. The decision to intervene is, of course, dependent on confounding factors, such as age or medical condition of the patient. Serial observation has been shown to be a safe, viable option in many cases with the advent of modern imaging techniques.
A large review was reported from the Mayo Clinic involving 217 patients with SAAs. Of these patients, 168 underwent nonoperative management for a mean period of 75 months.3 The mean size of the SAA in the nonoperative group was 2.1 cm, with a range from 0.8 to 5 cm in diameter. About half of these aneurysms were monitored with serial imaging; only 10% were noted to have growth averaging 0.06 cm/year. No rupture or other complications related to the SAAs occurred, and only 3 of the original 168 patients required intervention due to aneurysm growth. Similar results were reported by Lakin et al,77 who reviewed the Cleveland Clinic experience of 128 SAAs managed over a 15-year period. The observational cohort of 66 SAAs had a mean size of 1.7 cm at presentation, with a range from 0.8 to 4.2 cm. Serial imaging was available for 94% of the aneurysms, and these patients received an average of 2.5 CT scans during 4.6 years of follow-up. The average growth rate was a nominal 0.2 mm/year over 3.1 follow-up years. Again, there were no ruptures or other complications attributed to the aneurysms in the observed group.
Open Surgical Repair.
Options include complete resection with splenectomy, proximal and distal ligation of the aneurysm, or ligation with arterial reconstruction. To visualize the splenic artery, dissection proceeds with mobilization of the splenocolic ligament. The splenic flexure is then mobilized away from the retroperitoneum and abdominal wall. The aneurysm sac can be identified with palpation or ultrasound. Splenectomy is not uniformly needed because the short gastric vessels will adequately perfuse the organ after splenic artery ligation. Splenectomy is preferred for lesions adjacent to the splenic hilum or those involving the intrasplenic branches within the parenchyma. Laparoscopic repair should be complimented with the use of intraoperative ultrasound.85,86 Splenectomy, ligation, or aneurysmectomy have all been successfully performed by laparoscopic intervention.
The long-term results of open surgical repair for SAAs show a high survival and low complication rate, confirming the durability of the surgical approach.79 Marone et al79 reported a series of 34 SAAs treated with elective open surgical repair in which survival at 1 and 5 years were 100% and 92%, respectively.79 In the Mayo Clinic series, 49 patients underwent surgical intervention, 39 of whom had elective surgery. Operative mortality was 20% in the ruptured group and 5.1% in the elective group. Complications were low for the nonruptured group, with no reported aneurysm recurrence over a mean follow-up of 70 months.3 Pulli et al9 reported long-term results of splanchnic artery aneurysms that included open surgical treatment of 30 SAAs. In 28 of these cases, the aneurysm was completely resected. In 22 cases, the splenic artery was reconstructed with an end-to-end anastomosis, and in five patients, the distal location of the aneurysm required splenectomy. One death due to acute pancreatitis occurred in the perioperative period in a patient operated on for a giant inflammatory aneurysm; this patient did not have a history of pancreatitis. This was the only perioperative death in the entire study group, for an overall 30-day mortality rate of 1.8%. No aneurysm-related deaths occurred during long-term follow-up.
Endovascular Repair.
Endovascular therapy has emerged as an effective option in the management of SAAs. Treatment usually includes coil embolization, use of cyanoacrylate glue, or a combination of both. A Cleveland Clinic series reported the outcomes of 49 SAAs treated with endovascular intervention.77 Coil embolization was performed in 45 cases, in which 11 had glue used adjunctively. There was a 96% technical success rate in the initial procedure, with secondary intervention ultimately achieving desired results when needed. Complications included a femoral access site hematoma requiring operative drainage, and two brachial artery access site injuries. Splenic abscess was noted in three patients, who required re-intervention.
Postembolization syndrome (PES) occurred in an additional five patients. PES is a known complication of SAA embolization, and infarcts are common events, but these generally resolve without sequelae.125 Other selected series have reported similar success rates in the endovascular management of SAAs ranging from 90% to 100%.25,62,126,127 Covered stent repair is thought to be ideal for exclusion of the aneurysm and preservation of the splenic artery, and in theory will not lead to PES.128 The use of covered stents in treating SAAs remains limited to proximal lesions, and their use has not been as widespread as endovascular ablation. In the rare situation of a giant SAA, an endovascular intervention may precede an open repair in a staged procedure.65,129
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


