Chapter 61 Spine Exposure
Operative Techniques for the Vascular Surgeon
Surgery is the standard treatment for a multitude of benign and malignant disease processes of the spine. The anterior approach to the spinal column is important in degenerative disk disease, neural decompression, resection of neoplasms, trauma, infection, and congenital anomalies.1–4 Safe access to the spine is paramount to performing successful spinal procedures. Although orthopedic surgeons and neurosurgeons have been responsible for many surgical advances in spine surgery, access to the spine is often provided by vascular surgeons, general surgeons, urologists, or spine surgeons. With increasing frequency, vascular surgeons are the primary surgeons for anterior spine exposure owing to their skill and experience in retroperitoneal surgery. The operative techniques involved in retroperitoneal aortoiliac surgery can be modified to perform spine surgery. An experienced team approach to spine exposure can reduce intraoperative complications.1
The level of involvement by vascular surgeons varies by institution. Generally, vascular surgeons perform exposure of the lower thoracic, lumbar, and sacral spine levels. Thoracic surgeons are often involved in upper thoracic exposure, and the cervical spine is the domain of spine surgeons. The morbidity of the anterior approach has been reported to range from 10% to 30%.1,2 Periprocedure complications can include iatrogenic vascular, visceral, genitourinary, and neurologic injuries.1–4
Approach to the Thoracolumbar Junction
Operative Exposure
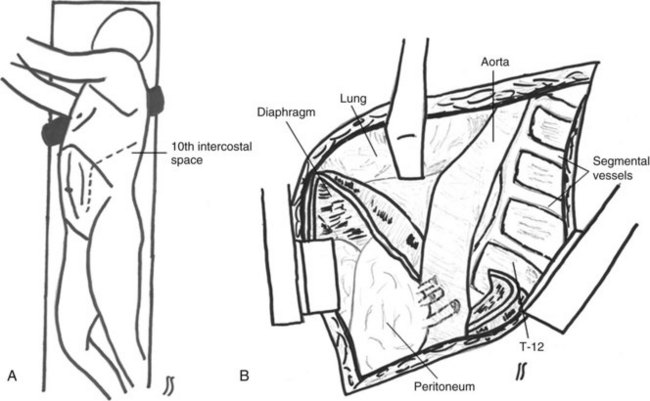
The rib space to be entered depends on the level of interest. In general, a curvilinear incision is made in the ninth or tenth interspace for access to the lower thoracic spine. The incision starts in the midaxillary line and extends anteriorly and inferiorly toward the umbilicus (Figure 61-1A). It is important to preserve the intercostal neurovascular bundle at the inferior aspect of the rib. Resection of the costal cartilage facilitates the exposure. The external oblique, internal oblique, and transversus abdominis muscles are divided. A plane is developed between the diaphragm and retroperitoneal space along the costal attachment of the diaphragm. Care must be taken with the diaphragm, which originates from the upper lumbar vertebrae, arcuate ligaments, and twelfth ribs and attaches to the lower six ribs and xiphoid. Dividing the diaphragm circumferentially minimizes injury to the phrenic nerve (see Figure 61-1B); this is facilitated with a reticulating intestinal stapler, which reduces bleeding from the diaphragmatic edge and aids in reapproximation of the diaphragm during closure. Use of a Finochietto or Omni retractor for rib separation maximizes visualization. An Omni retractor provides access to the vertebral bodies while protecting vital structures. The Omni post is generally attached to the right side of the table for a left-sided approach. The Omni retractor is positioned across the incision. A wide retractor is placed anteromedially to retract the peritoneum, ureter, and kidney in a medial position. This retractor will serve to protect these structures along with the aorta during vertebral manipulation by the spine surgeon. Three separate right-angle retractors are placed to retract the lung superiorly, the psoas muscle posteriorly, and the iliac vessels inferiorly. Placement of the retractors in these positions ensures adequate exposure and aids in the prevention of inadvertent injuries.
Lumbosacral Spine Exposure: Anterolateral Approach
Patient Position
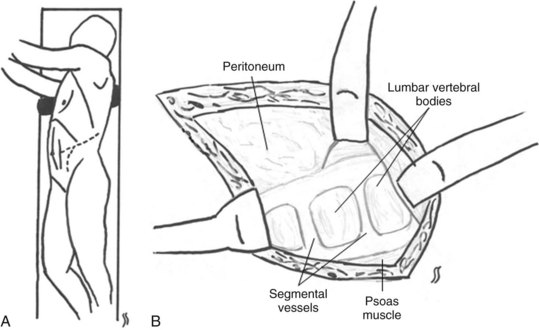
Similar to the thoracolumbar approach, the patient is positioned in a modified lateral decubitus position with the right side down to avoid the liver and injury to the vena cava. The hips are rotated 45 degrees. The upper and lower extremities are positioned in a similar fashion to the thoracolumbar approach (Figure 61-2A). The kidney rest is elevated, and the table is flexed to increase exposure between the lower ribs and the iliac crest.
Operative Exposure
An oblique incision is made over the eleventh rib from the lateral border of the quadratus lumborum to the lateral border of the rectus abdominis muscle for L1 and L2 exposure (see Figure 61-2A). For L3 to L5, a similar incision is made off of the twelfth rib. Electrocautery is used to divide the subcutaneous tissue, fascia, external and internal oblique, transversus abdominis, and transversalis fascia. The retroperitoneal space is entered laterally.
The peritoneal sac is swept off the anterior and lateral aspects of the abdominal wall, taking care not to violate the peritoneum. The peritoneum and kidney are reflected anteriorly. The peritoneum is dissected off the posterior rectus sheath, and the peritoneum is swept medially off the psoas muscle with Gerota’s fascia. The ureter should fall anteriorly with the peritoneum. The iliac vessels are exposed and protected. The psoas muscle is elevated bluntly off the lumbar vertebrae and retracted posteriorly. The lumbar segmental vessels are ligated as needed for exposure (see Figure 61-2B). Care should be taken to ligate the iliolumbar vein when dissecting the L4 to L5 level; this avoids avulsion of the vein during retraction. A spinal needle is inserted into the disk space, and a radiograph is taken to confirm the appropriate vertebral level.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


