Four patients are described with either parchment-like thinning or partial but extensive myocyte depletion with severe fatty or fibrofatty infiltration of the free wall of the right ventricle in its outflow tract, including 2 previously reported patients who also had focal parchment-like thinning of the left ventricular free wall. Three had documented ventricular tachycardia, and the remaining patient had sudden death as his first and only manifestation of heart disease. Three patients had severe heart failure: in 1, it was fatal, and the other 2 underwent cardiac transplantation. Necropsy cases of parchment-heart syndrome before 1980 are reviewed, as well as large series of cases with arrhythmogenic right ventricular dysplasia (ARVD) reported subsequently. It is suggested that ARVD is not an ideal name for this condition, because malignant ventricular arrhythmias are not universal, the left ventricular free wall and/or ventricular septum are sometimes involved, and the name “ARVD” neglects the fact that severe heart failure may be prominent in these patients. The right ventricular wall can be thin or parchment-like, or it may not be thinned but consist mainly of adipose tissue with or without focal fibrous tissue and a few islands of myocytes. Nevertheless, because the name “ARVD” has been commonly used and recognized for >30 years, it is probably best retained for this condition.
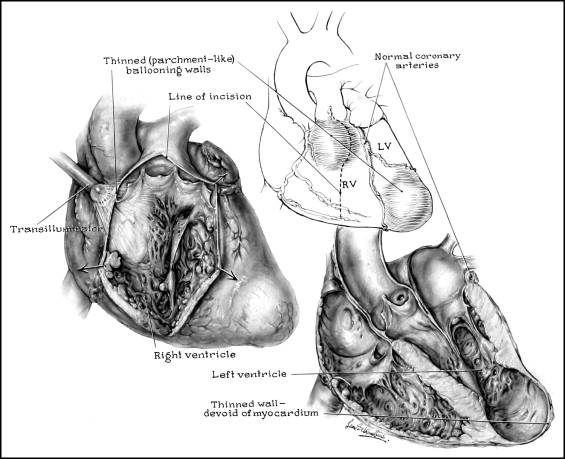
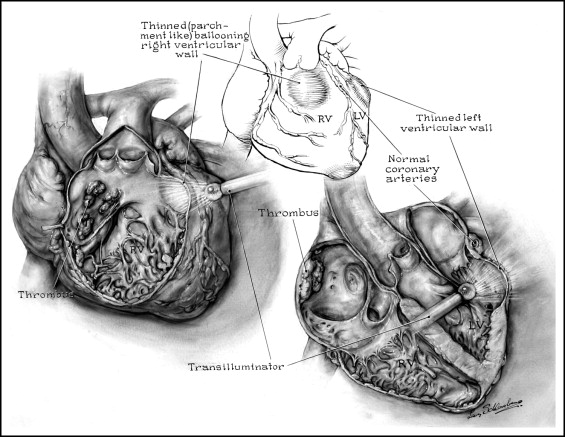
In 1905, Osler reported a man in his 40s who had died suddenly and unexpectedly while walking up a hill, and necropsy disclosed “parchment-like” thinning of portions of the right and left ventricular free walls in the absence of coronary narrowing or apparent cardiac valve dysfunction. In 1950, Segall described in more detail the patient briefly reported by Osler. The second patient reported (in 1952) to have a parchment-like heart was a 23-year-old woman who had chronic, eventually fatal heart failure and focal thinning of the walls of both ventricles. The third patient, a 7-year-old girl with severe right-sided heart failure and severe thinning of much of the right ventricular free wall, was described by Uhl, also in 1952. Thereafter, through 1980, ≥23 additional patients with parchment-like thinning of the right ventricular wall were reported ( Table 1 ). Except for the initial patient reported by Osler and later by Segall and 2 patients reported by Waller et al in 1980, all had myocardial wall thinning limited to the wall of the right ventricle. The 1 patient reported by Osler and later by Segall, the 1 patient reported by Castleman and Sprague, and the 2 patients reported by Waller et al all had congenital hypoplasia of portions of the right and left ventricular free walls in the absence of associated coronary or valvular heart disease. The term “arrhythmogenic right ventricular dysplasia” (ARVD) was first proposed by Fontaine et al in 1977 in a book chapter describing 6 patients with sustained ventricular tachycardia without heart failure and was put on the popular screen by Marcus et al in 1982. Since that time, numerous publications have appeared describing its clinical, radiographic, electrocardiographic, and hemodynamic features. The present report briefly describes again the 2 cases reported by Waller et al in 1980 and describes 2 additional patients, neither diagnosed clinically, with this syndrome treated by cardiac transplantation.
| Study | Age at Death | Gender | HF | Symptom Duration (months) | CE (X-Ray) | Abnormal Results on ECG | Mode of Death | HW (g) | Location of Thinned Ventricular Myocardium | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RV | LV | |||||||||||
| I | A | O | ||||||||||
| Patients aged ≤5 years | ||||||||||||
| Haworth et al (1975) | 1 day | M | + | 1/30 | + | + | HF | — | + | + | 0 | — |
| Diaz et al (1973) | 4 mo | M | + | 4 | + | + | HF | — | + | 0 | 0 | 0 |
| Novak et al (1957) | 5 mo | M | + | 5 | + | + | HF | — | + | + | 0 | 0 |
| Arcilla et al (1961) | 6 mo | M | + | 6 | + | + | HF | — | + | + | + | 0 |
| Uhl (1952) | 7 mo | F | + | 4 | + | + | HF | — | + | + | 0 | 0 |
| Cumming et al (1965) | 7 mo | F | + | 4 | + | + | PO | 48 | 0 | + | 0 | 0 |
| Aherne (1973) | 7 mo | F | + | 3 | + | + | HF | — | + | + | + | 0 |
| Perrin and Mehrizi (1965) | 10 mo | M | + | 7 | + | + | HF | — | 0 | + | 0 | 0 |
| Sherman (1963) | 15 mo | F | + | 12 | + | + | HF | — | + | + | + | 0 |
| Kinare et al (1969) | 60 mo | F | + | 60 | + | + | HF | 130 | + | + | + | 0 |
| Patients aged >15 years | ||||||||||||
| Abe et al (1973) | 17 yrs | F | + | 48 | + | + | PO | 400 | 0 | + | + | 0 |
| Murata et al (1976) | 18 yrs | F | + | 12 | + | + | HF | 400 | 0 | + | + | 0 |
| Froment et al (1968) | 19 yrs | M | + | — | + | — | HF | 350 | 0 | + | 0 | — |
| Vecht et al (1979) | 19 yrs | M | + | 132 | + | + | PO | 435 | + | 0 | 0 | — |
| Castleman and Sprague (1952) | 24 yrs | F | + | 12 | + | + | HF | 300 | + | + | + | 0 |
| Froment et al (1968) | 26 yrs | M | + | — | + | — | HF | 430 | 0 | + | 0 | — |
| Bharati et al (1978) | 29 yrs | F | + | 108 | + | + | HF+CHB | 545 | + | + | + | 0 |
| Osler (1905) (Segall [1950] ) | 40 s | M | — | — | — | — | SD | 168 | + | + | + | + |
| Reeve and MacDonald (1964) | 47 yrs | F | + | 432 | + | + | CVA | 290 | + | 0 | 0 | 0 |
| Forssman and Bjorkman (1972) | 47 yrs | M | 0 | — | — | + | SD | — | 0 | + | 0 | — |
| Gould et al (1967) | 66 yrs | M | 0 | 0 | 0 | 0 | L | 600 | + | + | 0 | 0 |
| Sugiura et al (1970) | 84 yrs | F | 0 | 0 | 0 | 0 | AP | 220 | 0 | 0 | + | 0 |
Patients Studied
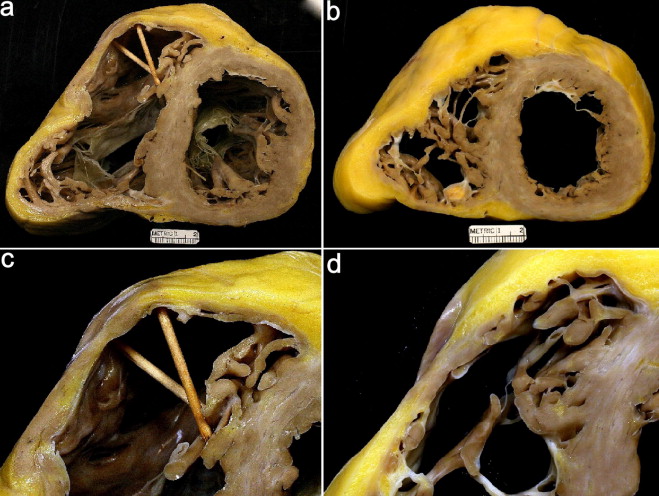
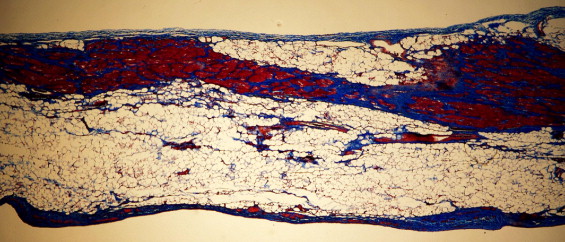
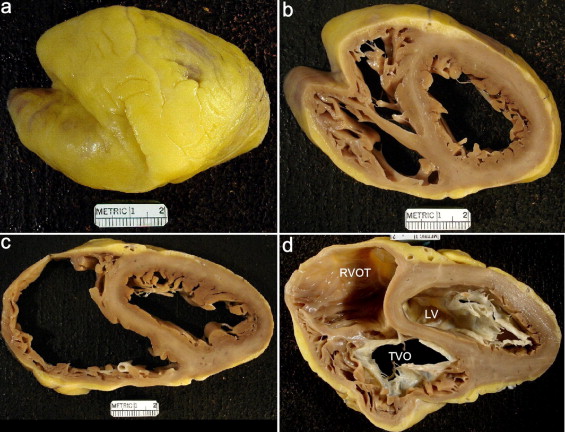
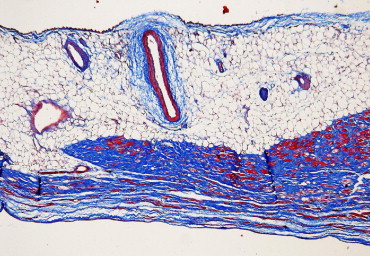
Pertinent clinical and morphologic features of the 4 patients are listed in Table 2 and illustrated in Figures 1 to 6 . One of the 2 earlier cases (patient 1) had severe, eventually fatal heart failure, and in the other (patient 2), sudden death was the first and only manifestation of his cardiac disease. Patients 3 and 4 had severe intractable heart failure and as a consequence underwent cardiac transplantation. Patient 2’s mother and sister had pacemakers. Patient 3 had ventricular tachycardia at 12 years of age treated by an ablation procedure, without recurrence thereafter. Patient 4 also had runs of ventricular tachycardia, and patients 3 and 4 underwent intracardiac defibrillator device insertion.
| Variable | Patient | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| Age (years) at death or CT | 61 | 55 | 26 | 44 |
| Gender | Male | Female | Male | Male |
| Age at symptom onset (years) | 61 | 53 | 12 | 42 |
| Heart failure, chronic | 0 | ++++ | ++++ | ++++ |
| Ventricular arrhythmia | — | + | + | + |
| Bundle branch block | — | + | + | + |
| Body mass index (kg/m 2 ) | — | 17 | 24 | 22 |
| Diagnosis of ARVD clinically | 0 | 0 | 0 | 0 |
| Clinical diagnosis | SD | Pericardial disease | IDC | HC |
| Intracardiac defibrillator implanted | 0 | 0 | + | + (2004) |
| Indirect blood pressure (mm Hg) | 130/70 | 115/80 ⁎ | 100/60 | 90/60 |
| 4-chamber dilatation | 0 | 0 | + | + |
| Pulmonary arterial pressure (mm Hg) (s/d) | — | 28/20 ⁎ | 50/30 (mean 38) | 19/12 (mean 14) |
| Cardiac index (L/min/m 2 ) | — | — | 0.8 | 1.9 |
| Ejection fraction (%) | — | 65 ⁎ | 15 | 25 |
| Heart weight (g) | 350 | 320 | 595 | 323 |
⁎ Cardiac catheterization was performed 21 months before death, and heart failure at that time was purely right sided.