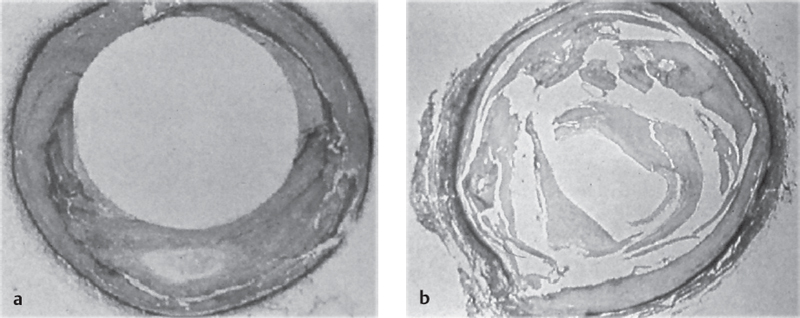
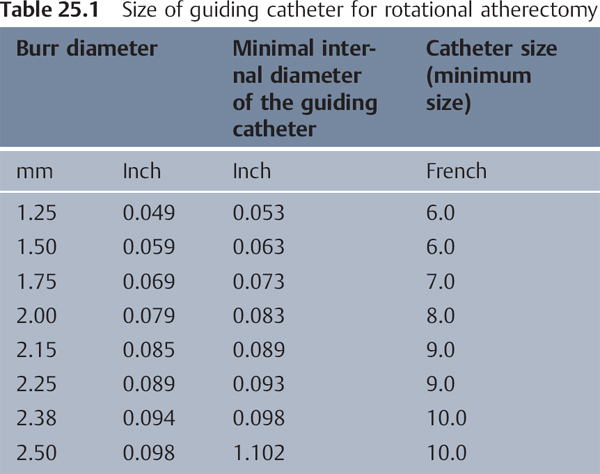
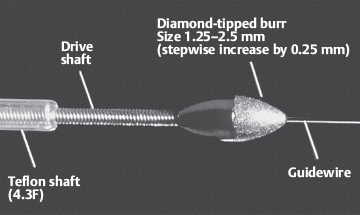
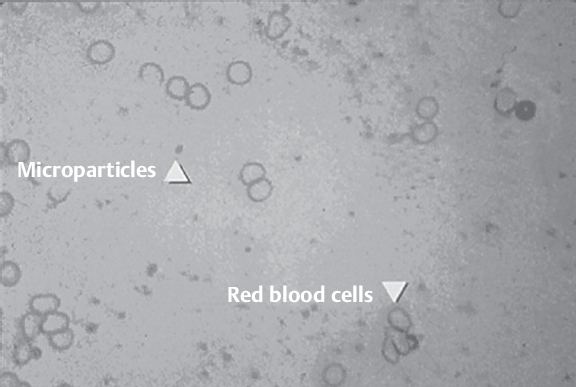
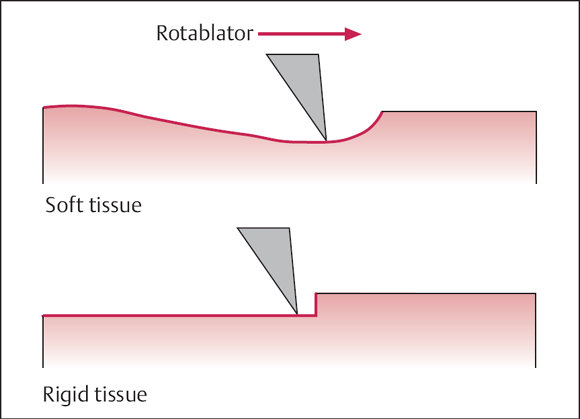
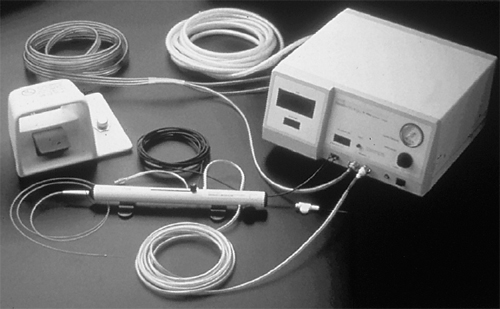
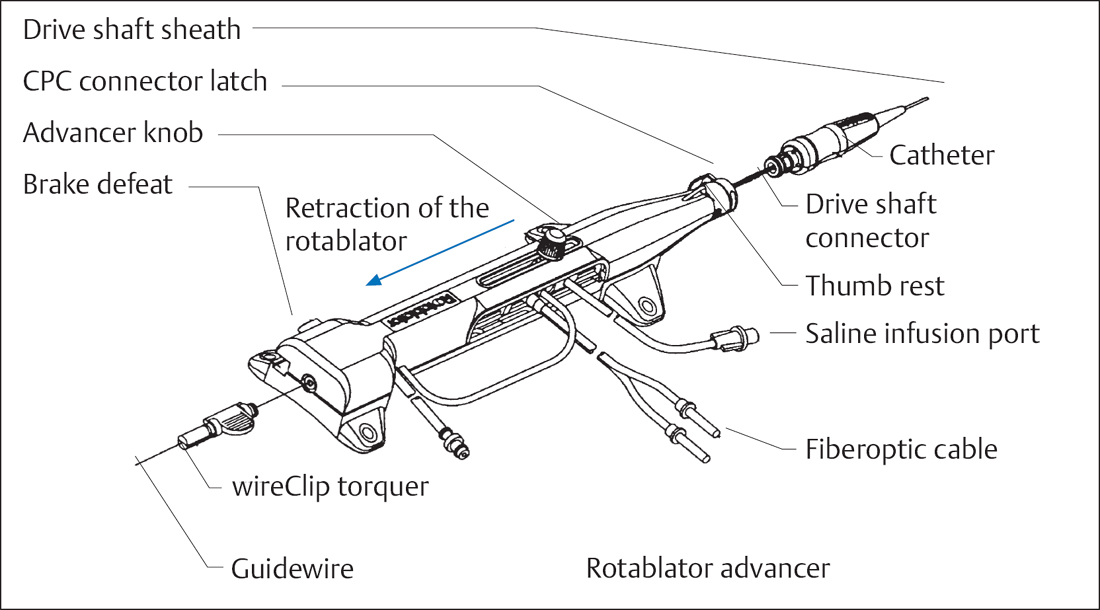
25 Rotational Atherectomy The principle of action of rotational atherectomy, or rotablation is the removal and the grinding of hard, calcified atherosclerotic material to remove a stenosis, rather than the compression or controlled dissection of the plaques as with balloon angioplasty. Currently, there is only one system available for rotational atherectomy (Rotablator Rotational Atherectomy System, Boston Scientific, Natick, MA, USA). A burr embedded with tiny diamond particles (Fig. 25.1) is rotated at 150,000 to 190,000 rpm by an external air turbine. Advancing the burr into the hard, rigid plaque produces very fine particles ~5 to 10 μm in size (Fig. 25.2), which are washed out into the coronary vascular bed and resorbed by the reticuloendothelial system. Elastic parts of the vessel evade the burr and thus are not injured (principle of differential cutting, Fig. 25.3). The aim of rotational atherectomy is the restoration of a smooth, circular vessel lumen without dissection (Fig. 25.4). Rotablation is not indicated for: Fig. 25.4 a, b Microscopic effects of rotational atherectomy vs. balloon angioplasty. a Restoration of smooth vessel lumen without dissection. b Extensive dissections after balloon angioplasty. Rotablator console with foot pedal (Fig. 25.5). This controls and monitors rotational burr speed. The Rotablator is connected to a compressed air or nitrogen supply. The rotational speed of the burr is changed by adjusting the turbine pressure (turning the knob). The console indicates not only the rotational speed but also the procedure time. The rotational speed is measured via a fiberoptic tachometer cable in the Rotablator (fiberoptic connection at the console). The foot pedal switches the gas turbine on and off; two frequency ranges can be selected: lower (“Dynaglide” mode) and higher rotational speed. Compressed air bottle and pressure controller. To run the turbine the console has to be connected to a gas bottle with pressure controller. The gas bottle with compressed air or nitrogen should hold at least 2,250 L (sufficient for ~20 minutes of operation). A backup bottle should be kept available. The gas flow is adjusted (at least 140 L/min at 0.65 to 0.75 MPa [6.5 to 7.5 bar]) with the pressure controller. Rotablator catheter. The Rotablator system consists of two parts; one is the drive unit (RotaLink Advancer), to which burrs of variable size can be connected. Advancer (drive unit). The housing of the drive unit contains the pressured air turbine and the rail to control the burr’s advance (Fig. 25.6). At the side of the housing are connections for the air supply, for the fiberoptic, and for flushing. A brake at the posterior end of the system fixes the guidewire during the ablation, so that it cannot spin or get out of place. The brake is automatically activated when the turbine is switched on. The burr can be exchanged together with the drive shaft. Burr. The ellipsoidal burr is coated on its anterior half with tiny diamond crystals (30–40 μm) and is attached to the tip of the flexible drive shaft (see Fig. 25.1). The drive shaft is protected by a 4F Teflon sheath, which is flushed during rotablation with normal saline to cool and lubricate the system. The burr is available in sizes between 1.25 and 2.50 mm. Guidewires. Diameter: shaft 0.009 in., tip 0.014 in. Length: 325 cm. There are three different types: The tips of the guidewires are radiopaque. The shafts of the wires, only weakly visible by fluoroscopy, consist of smooth, uncoated stainless steel. To direct the wires a special torque tool (wireClip Torquer) is used. The steerability of the wires is markedly reduced compared with standard wires. Guiding catheter. Standard PCI guiding catheters are used. The internal diameter of the catheter always has to be 0.004 in. (0.1 mm) larger that the maximal planned burr size. The respective sizes can be seen in Table 25.1. In addition to the general preparations for PCI, informed consent has to be obtained for the specific procedures and the typical complications of rotational atherectomy. Adjunctive pharmacotherapy. Depending on the laboratory, oral or parenteral pretreatment with a calcium channel blocker can be initiated to help prevent the relatively frequent vasospastic complications. Personal view We administer 1 to 2 mg nitroglycerin into the coronary artery immediately before the procedure, followed by additional intracoronary doses during the procedure. Also, the addition of verapamil and nitrates to the flush solution has proved useful (both 5 mg in 500 mL in normal saline; with a pressure of 300 mm Hg, 50 μg is infused in 30 seconds). The procedure depends on two different therapeutic strategies:
 Basics
Basics
 Indications
Indications
 Calcified stenoses
Calcified stenoses
 Complex coronary stenoses in angulated segments
Complex coronary stenoses in angulated segments
 Coronary stenosis or occlusions that can be crossed with a wire but not with a balloon
Coronary stenosis or occlusions that can be crossed with a wire but not with a balloon
 Rigid coronary stenoses that cannot be dilated
Rigid coronary stenoses that cannot be dilated
 Ostial stenoses (aorto-ostial or stenoses at the origin of large branches)
Ostial stenoses (aorto-ostial or stenoses at the origin of large branches)
 Bifurcation stenosis
Bifurcation stenosis
 Diffuse in-stent restenoses (?)
Diffuse in-stent restenoses (?)
 Stenoses in vein grafts (high restenosis rate, high risk of embolism)
Stenoses in vein grafts (high restenosis rate, high risk of embolism)
 Dissections, for example, immediately after balloon angioplasty, due to the risk that the dissection membrane/flap is wrapped around the burr. Wait 4 to 6 weeks before rotablation
Dissections, for example, immediately after balloon angioplasty, due to the risk that the dissection membrane/flap is wrapped around the burr. Wait 4 to 6 weeks before rotablation
 Ectatic coronary sclerosis: high thrombus burden, thin vessel wall
Ectatic coronary sclerosis: high thrombus burden, thin vessel wall
 Visible thrombi
Visible thrombi
 Known vasospasm
Known vasospasm
 Instruments
Instruments
 RotaWire Floppy: flexible guidewire with soft coil tip; the wire is usually located centrally in the vessel with only little vessel straightening
RotaWire Floppy: flexible guidewire with soft coil tip; the wire is usually located centrally in the vessel with only little vessel straightening
 RotaWire Floppy Gold: as above, with gold-coated tip for improved visibility
RotaWire Floppy Gold: as above, with gold-coated tip for improved visibility
 RotaWire Extra Support: stiff guidewire with longer soft tip and eccentric wire position and vessel straightening for angulated vessels
RotaWire Extra Support: stiff guidewire with longer soft tip and eccentric wire position and vessel straightening for angulated vessels
 Procedure
Procedure
Special Patient Preparation
Additionally, intracoronary heparin 10,000 to 12,500 IU.
Therapeutic Strategies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


