Fig. 10.1
The patient was positioned with the left chest elevated approximately 30° and with left arm tucked at the left side
10.2 Surgical Technique
After the expose of left chest, the endoscopic camera is inserted via a 0.8 cm incision in the 5th intercostal space (ICS) in anterior axillary line (AAL). The left and right instrument arms are inserted through two 0.8-cm trocar incisions in 3rd and 7th ICS in AAL. A 2-cm incision posterior to the camera in the 5th ICS in midaxillary line (MAL) of left side is used as working port for the introduction of the lead and sutures as necessary (Fig. 10.2). Carbon dioxide is continuously insufflated into the chest cavity via camera cannula and the CO2 insufflation at a pressure of 8–10 mmHg is used in the left pleural space to help with exposure. Special consideration has to be given to hemodynamic effects because of the impaired heart function.

Fig. 10.2
Port placement for robotic left ventricular epicardial lead placement. The ports are placed in line in AAL and the working port in MAL. The tip of the instrument is allowed for the access to the ventricular surface
The instruments are controlled by a surgeon who sits at the operating console away from the operative field. The pericardium is then opened posterior to the phrenic nerve (Fig. 10.3), the lateral and posterior left ventricular wall was exposed. As the patient has complete atrioventricular block, a temporary epicardial pacing lead is sutured (Fig. 10.4) and used as standby after it is tested working normally. A screw-in type epicardial pacing lead (Fig. 10.5) is introduced to the thoracic cavity through the working port by the patient-side surgeon (Fig. 10.6) then rotated into the lateral and posterior left ventricular wall with two laps (Fig. 10.7).
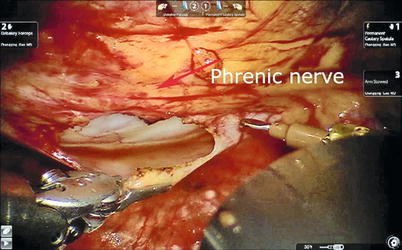
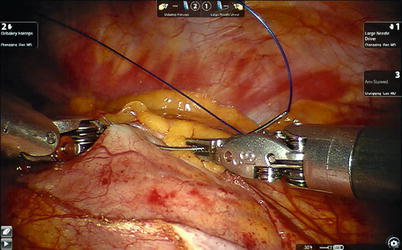
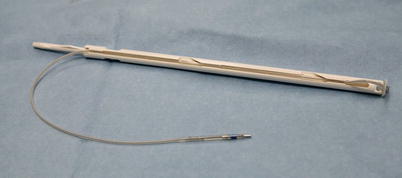

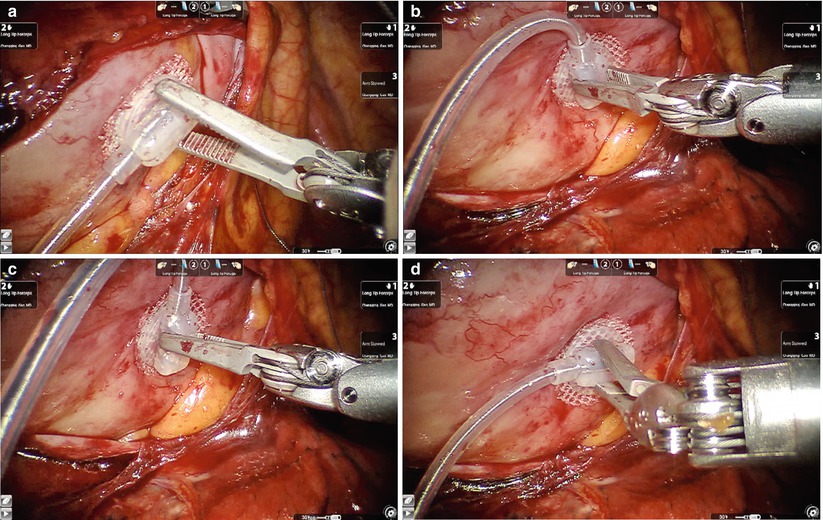
Fig. 10.3
The pericardium is opened posterior to the phrenic nerve
Fig. 10.4
The temporary epicardial pacing lead is sutured
Fig. 10.5
The MEDTRONIC screw-in type epicardial pacing lead
Fig. 10.6
The screw-in type epicardial pacing lead is delivered by the patient side surgeon
Fig. 10.7
The screw-in type epicardial pacing lead is rotated clockwise into the lateral posterior wall of the left ventricle from part (a) to part (d)
The robotic arms are used to fix the lead to the left ventricular surface by screw in fixation and the other end of lead is brought out through the right port (Fig. 10.8). The lead was tested for threshold, resistance, and lateness within the native QRS complex. A transverse incision is made at the pacemaker pocket and the previous dual chamber pacemaker is isolated and took out (Fig. 10.9), meanwhile the temporary pacemaker is working instead. The left ventricular epicardial pacing lead, which is then tunneled to the pacemaker generator pocket, together with the previous right ventricular lead and the right atrial lead are all connected to the three chambers pacemaker, and these are embedded in the pocket. After the pacemaker is confirmed working smoothly, the pocket as well as the chest incisions are sutured. A thoracic drainage tube was placed and the patient was transferred to ICU.




