Fig. 4.1
3-D CTA of iliac-femoral artery and abdominal aorta
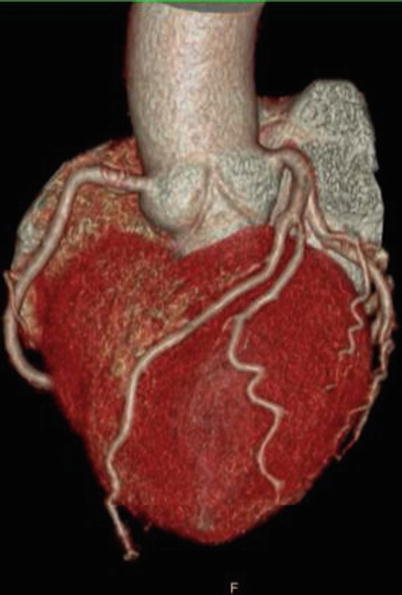
Fig. 4.2
3-D CTA of coronary artery
4.2 Preparation of Conduits of Peripheral CPB
The CPB conduits are specially designed for the peripheral CPB establishment at the PLA General Hospital. Venous conduit has two bifurcations, one is much shorter than the other so that these two conduits can be comfortably placed on the table after cannulation (Fig. 4.3).
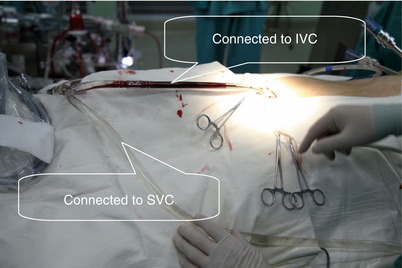
Fig. 4.3
Venous conduits placed on table
Proper size of cannula for femoral artery and vein cannulation is selected according to the weight and height of the patient. The surgeon’s experience is also of much importance for cannula selection. So far, 15 F cannula is routinely used for internal jugular cannulation at the PLA General Hospital, and the outflow is sufficient. For femoral vein cannulation, 23 F cannula is most frequently used. 21 F cannula is adequate for arterial inflow for patients with weight of about 80 kg. The lightest weight of the patient receiving robotic heart surgery performed at the PLA General Hospital was 29 kg, and the arterial cannula size was 17 F.
4.3 Techniques for Peripheral CPB Establishment
Intraoperative transesophageal echocardiography (TEE) plays a very important role in venous cannulation for peripheral CPB set up. The precise positioning of the internal jugular vein cannula and femoral vein cannula, which are both advanced into right atrium, must be guided by TEE.
After general anesthesia and double-lumen endotracheal intubation, a 15 gauge angio-catheter is inserted and secured in advance by anesthesiologist with the guidance of ECHO (Fig. 4.4) and heparin is infused inside the catheter (Fig. 4.5). The puncture site of skin for angio-catheter is just 10 mm above the clavicle. The puncture site of internal jugular vein should be guided by ECHO and be just at the anterior middle portion of the vein, which is important for subsequent smooth advancement of a 15 F cannula. Another 7 F double lumen catheter is also introduced more cephalically (Fig. 4.6).
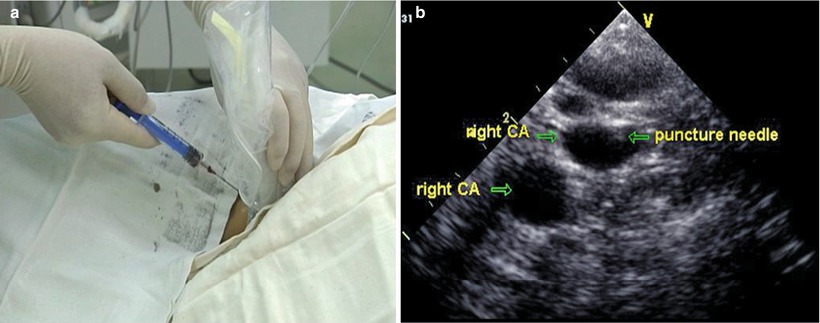
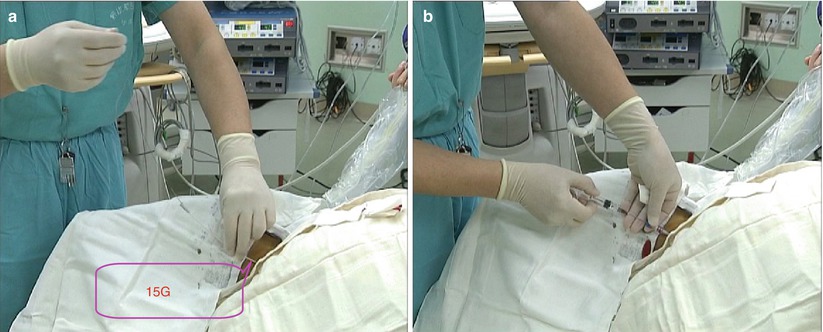
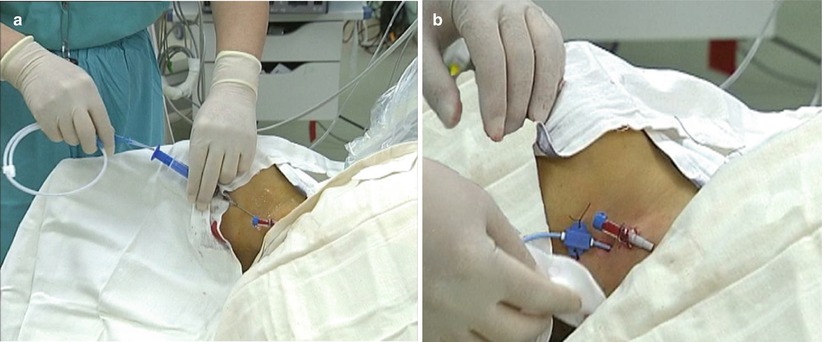
Fig. 4.4
Internal jugular cannula with guidance of ECHO. (a) To puncture the internal jugular vein under guidance of ECHO; (b) The EECHO view
Fig. 4.5
A 15G angio-catheter is pre-positioned 10 mm above clavicle (a) and heparin is infused (b)
Fig. 4.6
Another 7 F double lumen catheter is inserted cephalically
4.4 Exposure of Femoral Artery and Vein
The patient is positioned as described above, and followed by sterilization and draping. A 2-cm transverse right groin incision just above the crease is made to expose the femoral artery and vein. The two vessels are dissected just below, rather than above, the femoral canal. This maneuver can avoid injury of structures within femoral canal, and may not decrease the strength of the abdominal wall because the plane of dissection is just at the inferior edge, instead of within, the femoral canal (Fig. 4.7). A purse string with 5/0 polypropylene suture is placed at the anterior wall of the femoral vein. Two snares are placed around the femoral artery and vein respectively (Fig. 4.8).
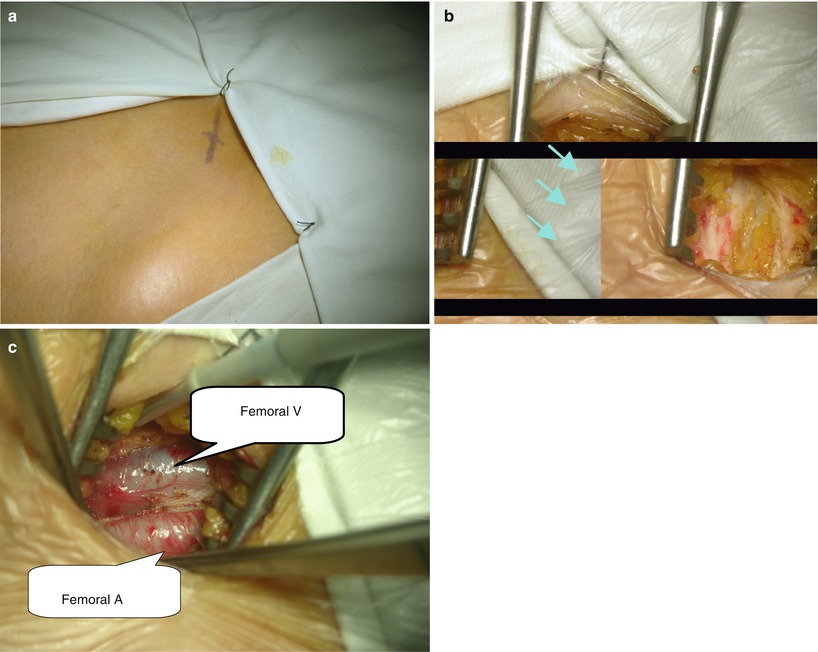

Fig. 4.7
Exposure of femoral artery and vein. (a) The skin mark of incision; (b) The dissection plane at the inferior edge of abdominal wall; (c) The dissected right femoral artery and vein
Fig. 4.8
(a) A purse string suture on the right femoral vein; (b and c) Two snares around right femoral artery and vein
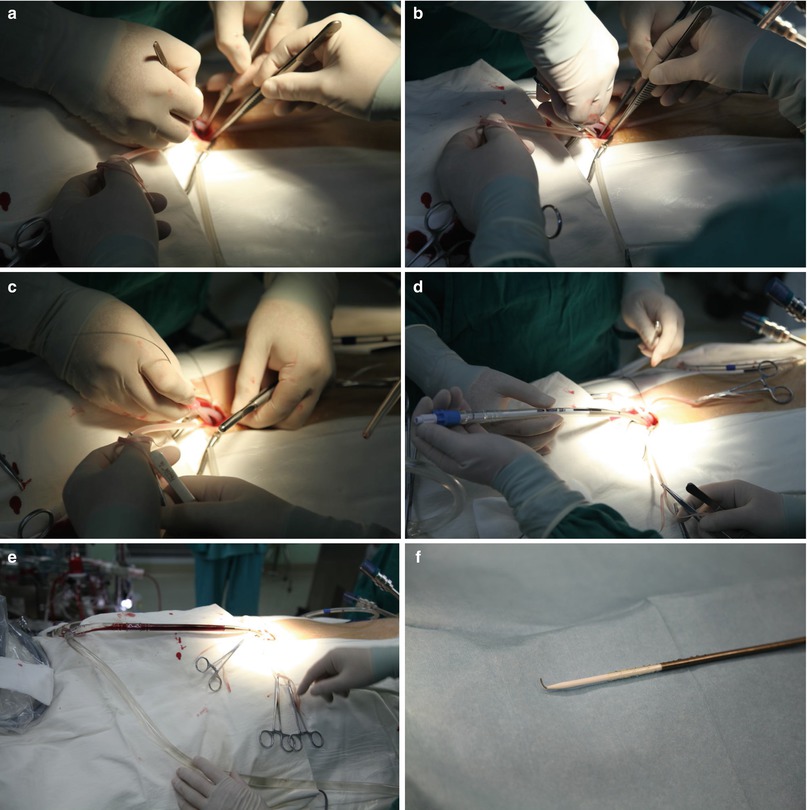
4.5 Femoral Artery Cannulation
After systemic heparinization (300 IU/kg), the femoral arterial is clamped with two fine clamps, between which transverse arteriotomy was made and the arterial cannula is inserted using the Seldinger guidewire method. The guidewire, which has been inserted within the cannula in advance, is firstly introduced into femoral artery. The guidewire should be passed into the artery smoothly without any resistance. Arterial cannula insertion along the guidewire is followed. Assistant should hold the end of the cannula tightly to facilitate the insertion of the tip of the cannula. The surgeon holds the tape and the cannula is carefully advanced into the artery for at least 10 cm deep along the guidewire. Femoral artery is then snared and the guidewire is withdrawn and the cannula is clamped by the assistant. Blood is allowed to squirt for de-airing and good blood flow is checked. Cannula is connected to the arterial conduit of CPB and secured with two sutures (Fig. 4.9).
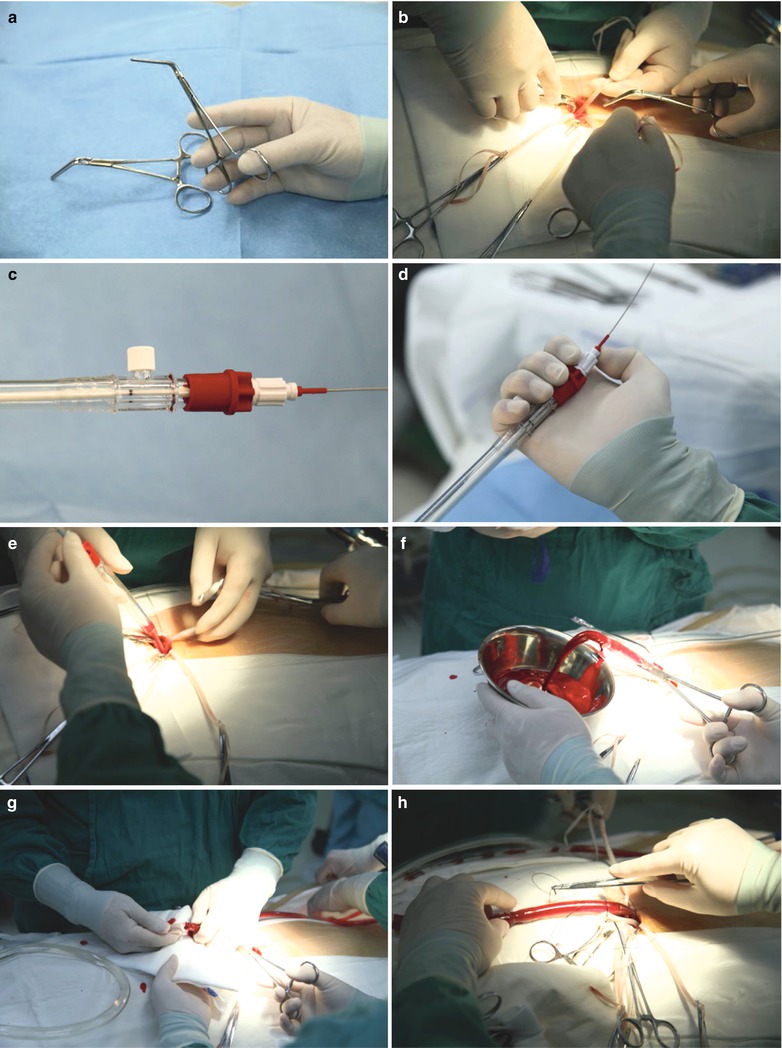
Fig. 4.9
(a–h) Femoral artery cannulation using Seldinger guidewire method. (a) The clamp for femoral artery occlusion; (b) The right femoral artery was occluded; (c) The end of femoral catheter; (d) The assistant hold the end of the cannula to facilitate the insertion of the tip of the cannula; (e) The cannula is advanced into the femoral artery; (f) Deairing and check the blood flow; (g) The cannula was connected to the arterial conduit of CPB; (h) The cannula was secured with two sutures
4.6 Femoral Vein Cannulation into the Right Atrium
Just after completion of arterial cannulation, TEE probe has already been standing by and focusing on the IVC to guide the venous cannula positioning. The two snares around femoral vein are pulled slightly and a small incision is created within the purse string suture. The small incision is dilated by mosquito clamp to facilitate venous cannula entrance. Seldinger guidewire is then advanced into right atrium under the guidance of TEE followed by venous cannula insertion. The venous cannula tip is positioned at the middle portion of right atrium. Care must be taken to clearly visualize the cannula passing through the SVC and into right atrium. The cannula is clamped and subsequently connected to venous conduit of CPB. Before the clamp is released, the other end of bifurcated venous conduit of CPB must be clamped to prevent bleeding (Fig. 4.10).