Right Ventricular Outflow Tract Obstruction
The right ventricular outflow tract includes the right ventricular outlet chamber (or the infundibulum); the pulmonary valve; the main, right, and left pulmonary arteries; and the peripheral pulmonary arterial branches. Obstruction can occur at a specific site or involve many segments of the right ventricular outflow tract. Obstruction of the right ventricular outflow tract is commonly associated with other cardiac anomalies.
Double-Chambered Right Ventricle
This consists of a hypertrophied muscle band creating obstruction between the inlet and infundibular portion of the right ventricle. An enlarged acute marginal branch of the right coronary artery often overlies the area of obstruction. Most often, a double-chambered right ventricle is associated with a perimembranous type of ventricular septal defect.
Technique for Repair
Cardiopulmonary bypass with bicaval cannulation is used. After aortic cross-clamping and cardioplegia delivery, a transverse right ventriculotomy is made just superior to the suspected obstructing muscle band (Fig. 23-1). This can be identified by an overlying enlarged coronary branch, external palpation of the right ventricle for a prominent ridge, or careful pressure measurements before beginning cardiopulmonary bypass. By retracting the inferior margin of the ventriculotomy, a circular opening can be seen, often covered with fibrous tissue. This obstruction is incised anteriorly initially. After identifying the papillary muscles of the tricuspid valve, the remainder of the obstructing muscle is resected. The accompanying ventricular septal defect should now be apparent. This ventricular septal defect may be closed through the right ventriculotomy or through a separate right atrial incision, working through the tricuspid valve (see Chapter 21). The right ventriculotomy is then closed with a running 5-0 Prolene suture.
The circular opening visualized through the right ventriculotomy may, on first examination, appear to be the ventricular septal defect. Care must be taken to identify the location of the tricuspid valve to avoid this mistake.
Tetralogy of Fallot
An anatomic anomaly consisting of a ventricular septal defect, right ventricular outflow tract obstruction with resultant right ventricular hypertrophy, and dextroposition of the aorta was described by Fallot in 1888. These children usually present with mild to moderate cyanosis and may have intermittent hypoxic spells.
The anatomy must be accurately defined to plan the management of these patients. Echocardiography can demonstrate the presence of additional ventricular septal defects, can usually delineate the initial course of the right and left coronary arteries, and can size the main and proximal right and left pulmonary arteries. Cardiac catheterization is reserved for those patients in whom the echocardiographic diagnosis is incomplete, when aortopulmonary collateral vessels are suspected, or for patients with previous palliative procedures.
Staged Approach
Several centers have reported satisfactory results with complete repair of tetralogy of Fallot in neonates. However, as
the long-term results of repair of tetralogy of Fallot become available, the significant problem of right ventricular failure and its causes are being elucidated. It is now believed that pulmonary regurgitation plays a major role in the development of right ventricular dysfunction. For this reason, some surgeons advocate a staged approach in patients who require surgery before 4 to 6 months of age. Patients who become symptomatic early in life or are ductal dependent tend to have small pulmonic valves and usually require a transannular patch. By performing an initial shunt procedure (see Chapter 18) and delaying definitive repair until the patient weighs at least 6 kg, the hope is that the native valve and/or annulus can be preserved.
the long-term results of repair of tetralogy of Fallot become available, the significant problem of right ventricular failure and its causes are being elucidated. It is now believed that pulmonary regurgitation plays a major role in the development of right ventricular dysfunction. For this reason, some surgeons advocate a staged approach in patients who require surgery before 4 to 6 months of age. Patients who become symptomatic early in life or are ductal dependent tend to have small pulmonic valves and usually require a transannular patch. By performing an initial shunt procedure (see Chapter 18) and delaying definitive repair until the patient weighs at least 6 kg, the hope is that the native valve and/or annulus can be preserved.
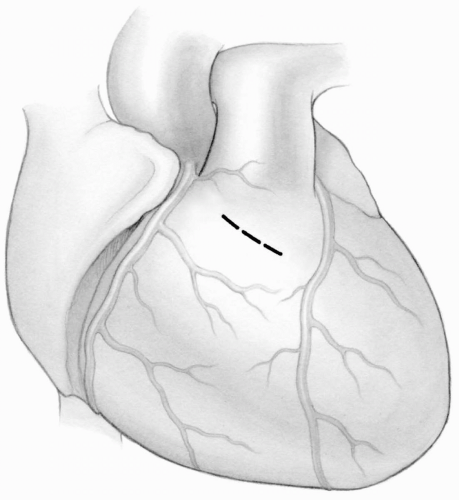 FIG 23-1. Transverse right ventriculotomy above enlarged coronary branch overlying muscle band. |
In addition, 3% to 5% of patients with tetralogy of Fallot have an anomalous left anterior descending coronary artery arising from the right coronary artery. The course of the left anterior descending coronary artery across the right ventricular outflow tract may preclude an appropriate ventriculotomy to relieve the obstruction. If these patients need surgery in the first few months of life, a shunt procedure is preferred. Some of these patients may be able to undergo a transatrial repair that is best performed in patients weighing at least 5 kg. However, many will require a right ventricular to pulmonary artery conduit as part of their repair, and this is best delayed until 12 to 18 months of age.
Technique for Complete Repair
A median sternotomy provides excellent exposure. A generous patch of autologous pericardium is harvested, attached with metal clips to a piece of plastic, placed in 0.6% glutaraldehyde solution for 6 to 8 minutes, and then rinsed in saline. Such treatment fixes the pericardium and thereby lessens the chances of aneurysmal dilation of the patch. If the patient has undergone a previous systemic to pulmonary shunt, it is dissected circumferentially to allow for closure with a metal clip at the initiation of cardiopulmonary bypass (see Chapter 18). In the absence of a shunt, minimal manipulation should be performed before cannulation to prevent hypoxic spells.
Besides confirming the anatomy with transesophageal echocardiography, an external examination of the heart is conducted. The surgeon looks for an anomalous coronary artery crossing the right ventricular outflow area, evaluates the size of the main and branch pulmonary arteries, and notes the distance between the aortic valve and the left anterior descending artery, which indicates the width of the right ventricular outflow tract. These observations help determine the surgical approach. A hypoplastic right ventricular outflow tract indicates the need for a right ventriculotomy and the probability of a transannular patch.
Standard bicaval and aortic cannulation is used to initiate cardiopulmonary bypass. A vent is placed through the right superior pulmonary vein into the left ventricle. Systemic cooling to 28°C to 32°C is achieved, the aorta is clamped, and cold blood cardioplegic solution is infused into the aortic root (see Chapter 3). In patients with discrete infundibular muscular obstruction and an adequate pulmonary annulus, the repair can be done through a transatrial approach.
Transatrial Technique
After achieving cardioplegic arrest, the tapes around the venae cavae are snugged down, and an oblique right atriotomy is made. The septal leaflet of the tricuspid valve is retracted to allow exposure of the ventricular septal defect and the right ventricular outflow tract. A cardiotomy sucker is placed in the infundibular ostium and dissecting scissors are used to resect muscle and fibrous tissue circumferentially. A right angle clamp is then used to identify hypertrophied muscle bands. With the clamp in place, each muscle band is divided with a no. 15 knife blade, cutting the band until the clamp is reached. The cut edge of the band can then be grasped with a forceps and resected with sharp scissors. When adequate resection of hypertrophied muscle has been completed, it should be possible to visualize the pulmonic valve (Fig. 23-2). A valvotomy can be performed by everting the leaflets and incising the commissures, if necessary. The annulus is sized with a Hegar dilator to ensure an adequate valve opening for the patient’s size (see Appendix section).
Care must be exercised when resecting muscle from the right ventricular outflow tract not to perforate the anterior wall. Checking outside the heart intermittently may be helpful. If a hole is created, it must be closed, usually with a pericardial patch (see subsequent text).
It is important to limit the resection of muscle along the anterior margin of the ventricular septal defect as this may compromise suturing of the patch to this edge.
The ventricular septal defect is closed with a patch of Dacron velour cut slightly larger than the defect. This can be secured in place with a continuous suture of 5-0 Prolene or multiple interrupted horizontal mattress 5-0 braided sutures with felt pledgets (see Chapter 21).
Transventricular Technique
Some surgeons prefer a right ventriculotomy approach for patients with tetralogy of Fallot. The advantages include the ability to resect all obstructing muscle bundles under direct vision and to enlarge an underdeveloped infundibulum with a patch. The potential disadvantages include scarring of the right ventricle, which may give rise to ventricular dysfunction and dysrrhythmias. Even when
a transventricular approach is used, every attempt is made to preserve the pulmonic valve leaflets and to avoid a transannular patch.
a transventricular approach is used, every attempt is made to preserve the pulmonic valve leaflets and to avoid a transannular patch.
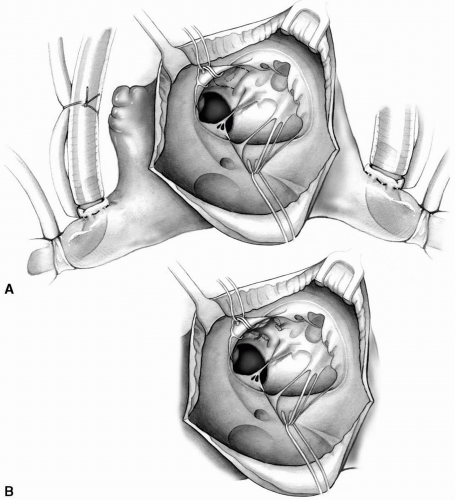 FIG 23-2. A: Exposure of ventricular septal defect and right ventricular outflow tract through tricuspid valve. B: Infundibular resection is complete and pulmonic valve can be seen. |
A vertical right ventriculotomy is made, and the edges are retracted with pledgeted sutures. The hypertrophied infundibular muscle bundles are incised and selectively excised as needed to open up the outflow tract (Fig. 23-3). The large malalignment type of ventricular septal defect can now be seen and is closed with a Dacron velour patch using a continuous suture of 5-0 Prolene. With this technique, traction on the patch by the assistant facilitates placement of the next stitch. Suturing begins at the 1 o’clock position and continues clockwise around the tricuspid annulus taking shallow bites of thickened endocardium up to the aortic annulus where the suture is tagged at the 8 o’clock position (Fig. 23-4). The other needle is then used to complete the suture line.
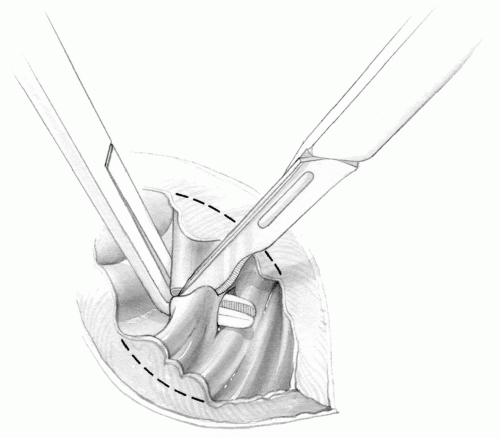 FIG 23-3. Transection of muscle band. Dotted line shows resection lines to excise hypertrophied muscle. |
To better preserve long-term right ventricular function, the length of the ventriculotomy should be limited to that needed to open the hypoplastic portion of the infundibulum.
If the right ventriculotomy must be extended to provide adequate exposure for closure of the ventricular septal defect, it is preferable to open the right atrium and close the ventricular septal defect through the tricuspid valve. Detachment of the anterior leaflet of the tricuspid
valve may be useful to expose the outlet portion of the defect (see Chapter 21).
valve may be useful to expose the outlet portion of the defect (see Chapter 21).
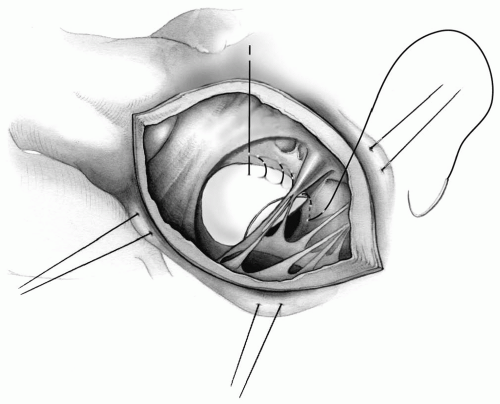 FIG 23-4. Continuous suture technique for the closure of ventricular septal defect through right ventriculotomy. |
When a right ventriculotomy is performed, muscle resection can be more limited because the patch itself will open up the outflow tract. Aggressive muscle resection leads to more endocardial scarring that may contribute to right ventricular dysfunction.
The aortic valve leaflets are immediately below the superior margin of the defect and can be punctured during suturing if deep needle bites are taken in this area (Fig. 23-5). Suturing in this area should therefore incorporate the crista marginalis, which holds sutures well.
The pulmonary valve and annulus are evaluated with Hegar dilators. Pulmonary valvotomy, if necessary, is carried out by bringing the pulmonary valve leaflets downward into the ventriculotomy.
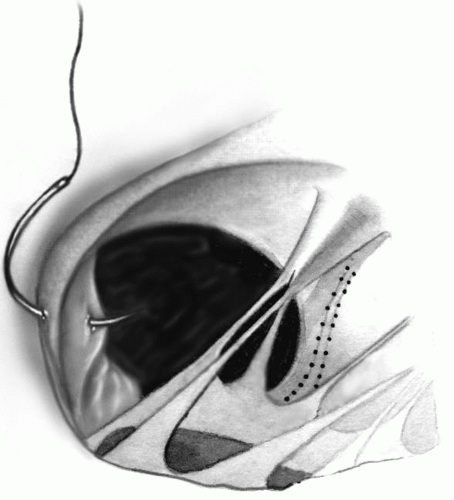 FIG 23-5. Proximity of an aortic valve leaflet to the rim of septal defect. |
Transpulmonary Approach to Pulmonic Valve and Annulus
Whether a transatrial or transventricular approach is used, evaluation of the pulmonic valve may be difficult working from below. In these cases, a separate vertical incision is made on the main pulmonary artery. Many surgeons prefer to use a transpulmonary approach to the pulmonic valve in all patients. After inspecting the valve and completing a valvotomy, if required, a Hegar dilator of the appropriate size is passed into the right ventricle (see Appendix section). If the annulus cannot be opened adequately with passage of sequentially larger dilators, the incision on the pulmonary artery is extended across the annulus only as far as necessary. This incision should be made through the anterior commissure of the pulmonic valve to reduce the amount of pulmonary insufficiency.
The transatrial-transpulmonary approach can be used in some patients with an anomalous coronary artery crossing the right ventricular outflow tract. In these cases, if transannular extension of the pulmonary arteriotomy is required, the incision must be made parallel to the anomalous vessel and an appropriately shaped patch used to maximize the opening of the right ventricular outflow tract (Fig. 23-6).
The orifices of the right and left pulmonary arteries are then evaluated. If stenosis of the take-off of the left pulmonary artery is noted, the pulmonary arteriotomy can be carried out onto the left pulmonary artery as far as
necessary to adequately relieve the stenosis. If narrowing of the right pulmonary artery is present, this may be best handled by extending the pulmonary arteriotomy onto the anterior surface of the right pulmonary artery behind the aorta. In this case, a separate rectangular patch is used to enlarge the opening of the right, or right and left pulmonary arteries (Fig. 23-7).
necessary to adequately relieve the stenosis. If narrowing of the right pulmonary artery is present, this may be best handled by extending the pulmonary arteriotomy onto the anterior surface of the right pulmonary artery behind the aorta. In this case, a separate rectangular patch is used to enlarge the opening of the right, or right and left pulmonary arteries (Fig. 23-7).
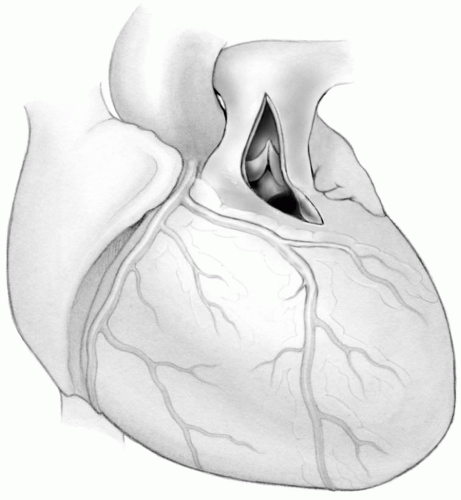 FIG 23-6. Pulmonary arteriotomy extended across annulus onto infundibulum parallel to anomalous coronary artery. |
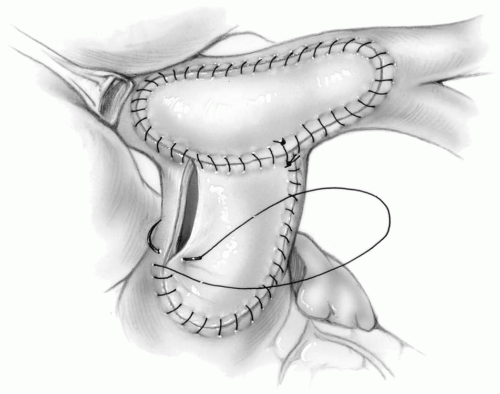 FIG 23-7. Two-patch technique to enlarge the proximal right and left pulmonary arteries. |
If the annulus is of adequate size, the pulmonary arteriotomy may be sutured primarily with a running 6-0 Prolene stitch, or closed with an appropriately sized patch of autologous pericardium to enlarge the main or left pulmonary arteries, as indicated. When used to enlarge the left pulmonary artery, the patch should be tailored with a squared-off end to provide optimal enlargement. The right ventriculotomy is then closed with an elongated oval patch of autologous pericardium or GORE-TEX, using a running 5-0 Prolene suture.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


