Radiation Pneumonitis
Presentation
A 72-year-old man presents with the chief complaint of shortness of breath. His symptoms have been progressive over the past year. He is able to climb two flights of stairs before having to stop and rest. His past medical history includes hypertension and hypercholesterolemia. In a review of systems, he denies chest pain, coronary artery disease, fever, cough, hemoptysis, or weight loss. He has an 80-pack-per-year history of smoking but quit 10 years ago.
The physical examination reveals a slender, pleasant gentleman in no respiratory distress. His vital signs are within normal range. The cardiac tones are normal, and his breath sounds are diminished throughout his lung fields. There is no cervical adenopathy. The rest of the examination is unremarkable. Basic laboratory studies revealed neither electrolyte abnormalities nor anemia.
Case Continued
Some of the differential diagnoses for shortness of breath include obstructive airway disease, parenchymal lung disease, and cardiogenic causes. Given the patient’s clinical symptoms, the following chest x-rays and computed tomography (CT) scans are obtained.
▪ Chest X-rays
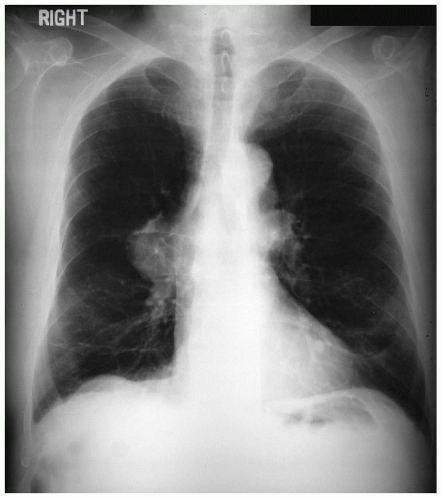 Figure 37-1 |
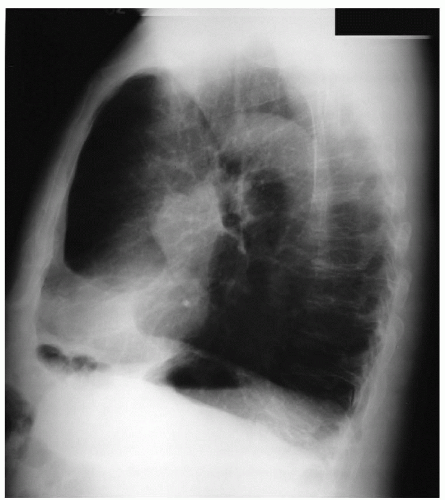 Figure 37-2 |
Chest X-ray Report
A large mass in the right hilar location is noted. The diaphragms are flattened, and the anteroposterior dimension is enlarged. There are no pleural effusions. The heart size is normal. ▪
▪ CT Scans
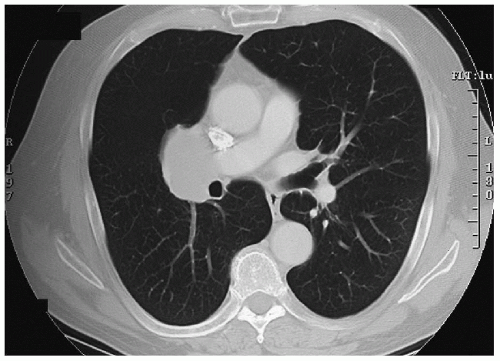 Figure 37-3 |
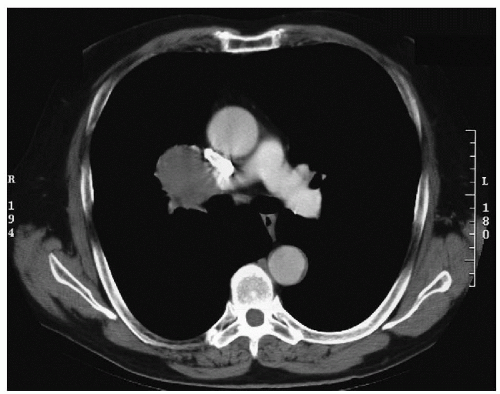 Figure 37-4 |
CT Scan Report
There is a large, lobulated, 6 cm × 4 cm soft tissue mass in the right hilar region in close proximity to the right upper lobe bronchus. There does not appear to be direct invasion into the superior vena cava or right main pulmonary artery, but the tumor is immediately adjacent to these structures. There are no other abnormal mediastinal or perihilar masses. There are no enlarged lymph nodes. There are no pleural or pericardial effusions.
Discussion
There are many types of lung masses, but a lesion such as this is most likely a bronchogenic carcinoma. A tissue diagnosis should be obtained. Because of the close proximity to the right upper lobe bronchus, bronchoscopy will most likely provide adequate tissue for analysis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


