We conducted a prospective study to determine whether a bolus injection of sodium bicarbonate before emergent coronary procedures in patients with chronic kidney disease (CKD) might prevent contrast-induced nephropathy (CIN). We enrolled 59 patients with CKD, defined by a serum creatinine concentration of >1.1 mg/dl or an estimated glomerular filtration rate of <60 ml/min, who were scheduled at admission to undergo an emergent coronary procedure. The patients were randomized to receive a bolus intravenous injection of 154 mEq/L of sodium bicarbonate (n = 30) or sodium chloride (n = 29) at the dose of 0.5 ml/kg, before contrast administration, followed by infusion of 154 mEq/L sodium bicarbonate at 1 ml/kg/hour for 6 hours in both groups. The primary end point was the occurrence of CIN, defined as an increase by >25% or >0.5 mg/dl of the serum creatinine level within 2 days after the procedure. In the sodium bicarbonate group, the serum creatinine concentration remained unchanged within 2 days of contrast administration (from 1.32 ± 0.46 to 1.38 ± 0.60 mg/dl, p = 0.33). In contrast, it had increased in the sodium chloride group (1.51 ± 0.59 to 1.91 ± 1.19 mg/dl, p = 0.006). The incidence of CIN was significantly lower in the sodium bicarbonate group than in the sodium chloride group (3.3% vs 27.6%, p = 0.01). In conclusion, rapid alkalization by bolus injection of sodium bicarbonate was effective for the prevention of CIN in patients with CKD undergoing emergent procedures.
Previous randomized studies investigating the prevention of contrast-induced nephropathy (CIN) with sodium bicarbonate reported that the hydration needed to be started 1 hour before the administration of contrast medium. In the clinical setting, we have often encountered patients requiring emergent coronary procedures, for whom, enough time to administer sufficient intravenous fluids for hydration could not safely be allowed. In contrast, in a study conducted of patients undergoing elective coronary procedures, a single bolus administration of sodium bicarbonate to patients with mild renal insufficiency undergoing an emergency coronary procedure was more effective for preventing CIN than standard hydration alone. However, no evidence has been available to date on the efficacy of bolus intravenous administration of sodium bicarbonate in patients with chronic kidney disease (CKD) undergoing emergent coronary procedures. Therefore, we performed a prospective randomized controlled trial to examine the efficacy of bolus injection of sodium bicarbonate administered before contrast injection for the prevention of CIN in patients with CKD undergoing emergent coronary procedures.
Methods
Consecutive eligible patients undergoing an emergent diagnostic or interventional coronary procedure, such as coronary angiography or percutaneous coronary intervention, at the Osaka General Medical Center were considered for enrollment. The indication for the emergent coronary procedure was suspected acute coronary syndrome in all cases. Eligible patients included those who were >20 years old and had renal insufficiency, defined by a serum creatinine (Cr) concentration of >1.1 mg/dl or estimated glomerular filtration rate (eGFR) of <60 ml/min, who were scheduled to undergo an emergent coronary procedure within 60 minutes of admission to our center. The eGFR was calculated using the following formula of the Japanese Society of Nephrology: 194 × Cr −1.094 × age −0.287 (× 0.739, for women). The exclusion criteria included a change in the serum Cr concentration of ≥0.5 mg/dl during the 24 hours before the procedure, pre-existing dialysis, exposure to the contrast media within 2 days before the study, allergy to the contrast media, pregnancy, and previous or planned administration of mannitol, fenoldopam, N -acetylcysteine, theophylline, dopamine, or nonstudy sodium bicarbonate. The ethics committee of our institute approved the study, and all the patients provided written informed consent before their participation in the study. The study was registered with ClinicalTrials.gov (Prevention of Contrast-induced Nephropathy by Sodium Bicarbonate Bolus Injection: NCT00700375 ).
Eligible patients were randomly assigned to the sodium bicarbonate group or the sodium chloride group in a single-blinded fashion. Randomization was performed with computer-generated random numbers. The patients received an intravenous bolus injection of 154 mEq/L of sodium bicarbonate (Meyron 84, 1 mEq/ml, Otsuka Pharmaceutical, Tokyo, Japan) or sodium chloride at a dose of 0.5 ml/kg, as soon as possible after they were admitted, before the administration of the contrast medium. Thereafter, both groups received an intravenous infusion of 154 mEq/L sodium bicarbonate at 1 ml/kg/hour during and for 6 hours after the coronary procedure. Thus, the osmotic pressure and intravenous fluid infusion volume were matched between the 2 groups. The fluids in either group were infused on an open-label basis; however, the patients and laboratory personnel processing the samples were unaware of the data and were unaware regarding to which group the patients had been randomized. The nonionic low-osmolality contrast medium, iopamidol (iopamiron 370, Bayer HealthCare, Osaka, Japan) or iohexol (Omnipaque 350, Daiichi Sankyo, Tokyo, Japan), was used in all the patients, and the volumes infused were left to the discretion of the operator. For most of the patients, the emergent coronary procedure was performed using the femoral approach. The decision to use an intra-aortic balloon pump or drugs was determined from the international guidelines and left to the discretion of the attending physician.
The serum Cr and blood urea nitrogen concentrations in venous blood samples were measured at baseline, on days 2 and 3 after the procedure, and at discharge. The left ventricular ejection fraction was evaluated using M-mode echocardiography for all the patients at entry. Chest radiography was performed at entry and on the morning of days 2 and 3 after the coronary procedure. The primary end point was the occurrence of CIN, defined as an increase by >0.5 mg/dl or >25% of the serum Cr concentration greater than the baseline within 2 days of the procedure. The patients were followed up during hospitalization, and any clinical events were recorded.
Before the present study, we calculated the sample size on the basis of power analysis, assuming the primary end point would occur in 22% of the patients in the sodium chloride group and 2% of the patients in the sodium bicarbonate group, as determined from the protocol of a previous study. It was projected that the inclusion of 40 patients in each group would yield a statistical power of 80%, with a type I error of 0.05. Continuous data are expressed as the mean ± SD. The categorical data were analyzed as absolute values and percentages. The tests of significance used were the t test for continuous variables and the chi-square test or Fisher’s exact test for the categorical variables. Repeated measures analysis of variance was used to compare the variables at baseline and after administration of the contrast medium between the 2 groups. A multivariate logistic regression model was used to determine the independent clinical factors associated with the development of CIN. p Values of <0.05 were considered statistically significant. All analyses were conducted using StatView J-5.0 (SAS Institute, Cary, North Carolina). Before achieving the planned number of study patients, we stopped enrollment because of the ethical concern of the continuing allocation of patients to the sodium chloride group, which was revealed to be associated with a greater risk of CIN after a review of the data.
Results
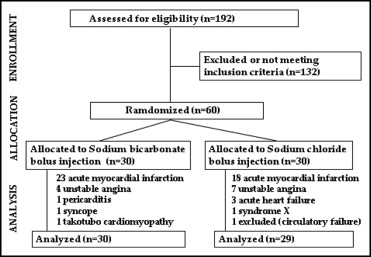
From June 1, 2008 and February 30, 2010, 192 patients were admitted to our center and underwent emergent coronary procedures. Of these, 60 patients fulfilled the criteria for inclusion in the study and were enrolled. However, 1 patient in the sodium chloride group was excluded. The study protocol had not been followed in this patient because of circulatory failure requiring rapid infusion at the coronary procedure. The number of patients who were randomly assigned to the 2 groups and their clinical diagnoses are presented in Figure 1 . All study patients had an eGFR of <60 ml/min. No significant differences were found in the baseline characteristics, parameters measured during the procedure, or drugs administered during the first 2 days of hospitalization between the 2 groups ( Table 1 ). Similar drugs were administered to the 2 groups during the study period.
| Variable | Sodium Bicarbonate (n = 30) | Sodium Chloride (n = 29) | p Value |
|---|---|---|---|
| Age (years) | 77 ± 9 | 75 ± 10 | 0.52 |
| Men | 23 (77%) | 23 (79%) | 0.81 |
| Body weight (kg) | 54 ± 13 | 60 ± 15 | 0.1 |
| Serum creatinine concentration (mg/dl) | 1.32 ± 0.46 | 1.51 ± 0.59 | 0.17 |
| Serum urea nitrogen (mg/dl) | 24.0 ± 10.5 | 26.0 ± 9.0 | 0.42 |
| Estimated glomerular filtration rate (ml/min) | 42.4 ± 11.5 | 38.7 ± 12.6 | 0.25 |
| Left ventricular ejection fraction (%) | 52 ± 14 | 57 ± 12 | 0.12 |
| Heart failure | 7 (24%) | 8 (28%) | 0.94 |
| Diabetes mellitus | 3 (10%) | 6 (20%) | 0.46 |
| Diabetes mellitus treated with insulin | 1 (3%) | 4 (13%) | 0.15 |
| Unstable angina pectoris | 3 (10%) | 7 (24%) | 0.15 |
| Acute myocardial infarction | 23 (79%) | 17 (62%) | 0.24 |
| Peak creatinine kinase in acute myocardial infarction (IU/L) | 2,379 ± 2,277 | 2,347 ± 2,414 | 0.97 |
| Interval from door to bolus injection (min) | 38 ± 14 | 37 ± 11 | 0.81 |
| Interval from bolus injection to contrast injection (min) | 11 ± 9 | 13 ± 8 | 0.54 |
| Volume of contrast media (ml) | 116 ± 63 | 104 ± 57 | 0.45 |
| Iopamidol (%) | 96.7 ± 0.18 | 93.1 ± 0.25 | 0.54 |
| Performed with percutaneous coronary intervention | 24 (80%) | 21 (72%) | 0.5 |
| Supported by intra-aortic balloon pump | 6 (20%) | 4 (14%) | 0.53 |
| Drugs administered ≤2 days after admission | |||
| Catecholamine | 9 (30%) | 6 (21%) | 0.65 |
| Aspirin | 26 (87%) | 27 (93%) | 0.1 |
| Statin | 9 (30%) | 4 (14%) | 0.12 |
| β Blocker | 22 (73%) | 21 (72%) | 0.94 |
| Angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers | 24 (80%) | 18 (62%) | 0.13 |
| Spironolactone | 4 (13%) | 1 (3%) | 0.18 |
| Loop diuretics | 13 (43%) | 16 (55%) | 0.37 |
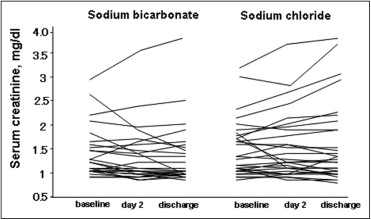
The course of changes in the serum Cr concentration in each patient and the postprocedural data are presented in Figure 2 and Table 2 , respectively. No significant increase was seen in the average serum Cr concentration from baseline to within 2 days of the procedure in the sodium bicarbonate group (from 1.32 ± 0.46 mg/dl before the contrast injection to 1.38 ± 0.60 mg/dl after, p = 0.33). In contrast, the average serum Cr concentration significantly increased within 2 days after contrast administration in the sodium chloride group (from 1.51 ± 0.59 mg/dl before the contrast injection to 1.91 ± 1.19 mg/dl after, p = 0.006). Furthermore, the serum Cr concentration in the sodium chloride group remained high even at discharge (p = 0.01). A significant difference in the serial serum Cr concentrations between the 2 groups was demonstrated by repeated measures analysis of variance (p = 0.02). The incidence of CIN was significantly lower in the sodium bicarbonate group than in the sodium chloride group (1 [3.3%] vs 8 [27.6%], risk ratio 0.12, 95% confidence interval [CI] 0.016 to 0.91, p = 0.01). To examine whether the randomization to the sodium bicarbonate group was independently associated with the decrease in the incidence of CIN, we entered the previously reported risk factors for CIN and the randomization to the sodium bicarbonate group in a multivariate logistic regression model ( Table 3 ). Randomization to the sodium bicarbonate group was independently associated with a reduction in the incidence of CIN.
| Variable | Sodium Bicarbonate (n = 30) | Sodium Chloride (n = 29) | p Value |
|---|---|---|---|
| Serum creatinine concentration day 2 after procedure (mg/dl) | 1.38 ± 0.60 | 1.91 ± 1.19 | 0.04 |
| Increase in serum creatinine concentration | |||
| From baseline to day 2 (mg/dl) | 0.06 ± 0.33 | 0.39 ± 0.69 | 0.02 |
| >0.5 mg/ml (n) | 2 (6.7%) | 8 (27.6%) | 0.01 |
| >25% (n) | 2 (6.7%) | 8 (27.6%) | 0.01 |
| Decrease in estimated glomerular filtration rate | |||
| From baseline to day 2 (%) | 1.31 ± 18.4 | 10.3 ± 25.0 | 0.12 |
| >25% (n) | 3 (10.0%) | 5 (17.2%) | 0.24 |
| Serum creatinine concentration at discharge (mg/dl) | 1.33 ± 0.43 | 1.94 ± 1.13 | 0.01 |
| Hospital stay (days) | 22.8 ± 17.9 | 21.4 ± 19.6 | 0.78 |
| Contrast-induced nephropathy ⁎ (n) | 2 (3.3%) | 8 (27.6%) | 0.01 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


