Positron emission tomography (PET) is the most selective and sensitive (picomolar to nanomolar range) imaging technique for measuring molecular pathways and interactions in vivo. Positron-emitting isotopes are radioactive variants of elements naturally occurring in organic molecules and can be incorporated without changing the chemical and biological characteristics of the labeled molecule. They decay by emission of a positron, which is the subatomic, positively charged, antiparticle of the negatively charged electron. The positron will annihilate with an electron and create two 511-keV photons, emitted in opposite directions. The detection of numerous of these annihilations by the detector rings of the PET camera generates high-resolution pictures (5 to 10 mm) indicating the sites of tracer accumulation in the body.
The most frequently used tracer in PET oncology is the glucose analogue 18 F-fluorodeoxyglucose (FDG). Its use is based on the increased glycolysis of cancer cells compared with normal tissues. This increased glycolysis is linked to an increase in glucose membrane transporters and upregulation of the principal enzymes that control the glycolytic pathway.1 FDG uptake is, however, not specific for cancer cells, and increased FDG uptake is also seen in some i nflammatory conditions, the most common cause of falsepositive FDG-PET findings.2 The ability to perform wholebody imaging within one examination makes PET an ideal technique for cancer staging. In clinical oncology, the FDG uptake is often quantified as the standardized uptake value (SUV; i.e., the ratio of the activity in tissue per unit volume to the injected dose per patient body weight). In vitro studies demonstrated that the amount of FDG uptake in tumor tissue is mainly related to the number of viable cancer cells3 and their proliferation capacity.4 Therefore, SUV changes on FDG-PET can be used to evaluate treatment efficacy, because tumor cell kill results in a proportional reduction of the FDG signal.5 Furthermore, the correlation between FDG uptake and proliferation capacity allows in vivo evaluation of tumor aggressiveness.
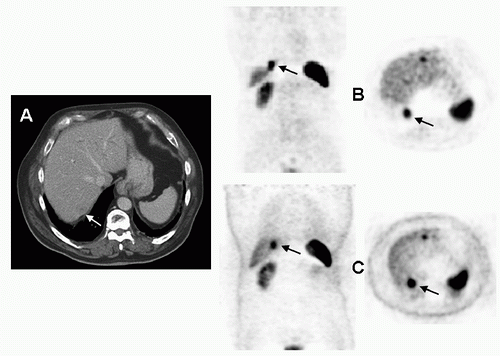
Interpretation of PET scans is hampered by the lack of anatomical detail, which makes it sometimes difficult to correctly localize hot spots or differentiate tumor tissue from benign structures with physiologically high FDG uptake (e.g., muscle, brown fat, gut). Therefore, PET always has to be interpreted in conjunction with anatomical images such as computed tomography (CT). Attempts to align or coregister CT and PET data sets acquired on separate machines with fusion software are generally only successful in the brain, whereas in the remainder of the body differences in patient setup present a challenge to the software approaches. Recently, integrated PET/CT systems were introduced, which enable acquisition of PET and CT data in the same session without changing the patients’ position. Since the installation of the first clinical PET/CT in 2001, the technology has gained widespread use and all new PET scanners installed today are integrated PET/CT machines. Another advantage of PET/CT is the possibility to use the CT component for attenuation correction of the PET images and reduce the scan time substantially (-50%), but specific artifacts can sometimes be a problem. 6 An example are the errors in localization of lesions caused by breathing and the difference in scan time to acquire a PET (minutes) and CT image (seconds). This can result in incorrect anatomical localization of lesions near the diaphragm on the attenuation-corrected images (Fig. 27.1). High-density objects (dental fillings, chemotherapy ports, barium contrast) can lead to an overestimation of tracer uptake, thereby producing false-positive PET findings. Therefore, non-attenuation-corrected PET images, which do not manifest these errors, should always be reviewed in parallel to recognize these artifacts.
Although FDG has made the way for PET in clinical oncology, several other radiopharmaceuticals can be used to study processes such as blood flow (H215 O), hypoxia (18 F-MISO), DNA synthesis (18 F-fluorothymidine [FLT]), and somatostatin receptor expression (Ga-68 DOTATOC). Certainly, with the rapid development of molecular-targeted treatments, noninvasive assessment of metabolic processes will become increasingly important to assess efficacy of these drugs. However, in the succeeding text, PET always refers to FDG-PET, unless otherwise specified. It summarizes the standard indications, other applications, and innovative use of this imaging technique (Table 27.1).
FIGURE 27.1 Ga-68 DOTATOC scan of patient with a typical carcinoid of the left lung (not shown). Existing liver metastasis were rather difficult to discern on the portal phase of CT (A), but Ga-68 DOTATOC PET proved to be a valuable adjunct to establish the liver lesion (B,C). Misalignment of PET and CT caused by breathing introduced attenuation artifacts and caused erroneous projection of the liver metastasis in the base of the right lung on attenuation-corrected (AC) PET images (B). Therefore, non-AC images (which do not harbor these artifacts) should always be reviewed (C).
Interpretation of PET Images If the aim of the PET study is just to stage the patient, visual analysis of non-a ttenuation-corrected images (i.e., hot spots higher than background activity being regarded positive for tumor) is probably just as good as SUV images, as has been pointed out by different prospective studies, both for the discrimination of nodules as well as for the evaluation of mediastinal involvement.7
There is a low degree of physiologic uptake of FDG in thoracic structures, including the lung, the heart, the aorta and large arteries, esophagus, thymus, trachea, thoracic muscles, bone marrow, and joints and soft tissues. This low background tracer activity builds the image contour. The high degree of FDG uptake in the brain and the excretory system impedes sensitive detection in these organs.
False-negative results may be lesion or technique dependent (Table 27.2). A critical mass of metabolically active malignant cells is required for PET detection. 8 Interpretation should be careful in tumors with decreased FDG uptake such as very well-differentiated adenocarcinoma, bronchioloalveolar carcinoma, or carcinoid tumors. FDG-avid lesions smaller than 5 mm may be false negative because of the limitations in spatial resolution of the PET scanner and partial volume effects in small lesions. In the lower lung fields, the detection limit may even go up to 10 mm as a result of additional respiratory motion. Factors inherent to the technique are paravenous FDG injection or high-baseline glucose serum levels. Blood glucose levels should be checked, and it is advised to proceed only if the glucose level is within a normal range prior to tracer injection. Although diabetic patients were often excluded in prospective studies, FDG uptake is probably not significantly influenced in these patients if the blood glucose levels are reasonably controlled.
Table 27.1 Applications of FDG-PET Scan in Lung Cancer
Diagnosis of Pulmonary Nodules and Masses
Differentiation of malignant vs. benign nodules
Reduce the need of unwanted invasive procedures
Aid in decision algorithms
False positives
Inflammatory respiratory disorders
False negatives
Small tumors (<8-10 mm)
Tumors with low glucose metabolism
Mediastinal LN staging
High negative predictive value for LN metastasis
Reduce the number of invasive tests, without loss of accuracy
Better guidance of invasive procedures
False positives
Inflammatory LNs
False negatives
Low FDG uptake in primary tumor
LNs obscured by centrally located tumors or hilar nodes
Extrathoracic Staging
Complement to conventional imaging
Detection of unexpected metastasis
Characterization of equivocal lesions
False positives
Inflammatory lesions
Second primary tumor
False negatives
Low FDG uptake in primary tumor
Small metastatic deposits
Other Applications
Prognosis (independent from TNM stage)
Early response evaluation during chemotherapy
Reassessment after induction treatment
Planning of radiotherapy
Diagnosis of recurrence after radical therapy
Selective use in lung cancer screening
Innovative Indications
Use of tracers other than FDG
Improvements in PET/CT cameras
Response evaluation in molecular therapy
Table 27.2 Caveats in the Interpretation of PET in Lung Cancer Patients
Causes of False-Negative Findings
Lesion dependent
Small tumors (<8-10 mm)
Ground-glass opacity neoplasms (BAC)
Carcinoid tumors
Technique dependent
Hyperglycemia
Paravenous FDG injection
Excessive time between injection and scanning
Causes of False-Positive Findings
Infectious/Inflammatory lesions
(Postobstructive) pneumonia/abscess
Mycobacterial or fungal infection
Granulomatous disorders (sarcoidosis, Wegener)
Chronic nonspecific lymphadenitis
(Rheumatoid) arthritis
Occupational exposure (anthracosilicosis)
Bronchiectasis
Organizing pneumonia
Reflux esophagitis
Iatrogenic causes
Invasive procedure (puncture, biopsy)
Talc pleurodesis
Radiation esophagitis and pneumonitis
Bone marrow expansion postchemotherapy
Colony-stimulating factors
Thymic hyperplasia postchemotherapy
Benign mass lesions
Salivary gland adenoma (Whartin)
Thyroid adenoma
Adrenal adenoma
Colorectal dysplastic polyps
Focal physiological FDG uptake
Gastrointestinal tract
Muscle activity
Brown fat
Unilateral vocal cord activity
Atherosclerotic plaques
BAC, bronchioloalveolar cell carcinoma.
False-positive findings are a result of the fact that FDG uptake is not tumor specific, and can be found in all active tissues with high glucose metabolism, in particular inflammation (Table 27.2). Therefore, clinically relevant FDG-positive findings, especially if isolated and decisive for patient management, require confirmation. The differentiation between metastasis, a benign or inflammatory lesion, or even an unrelated second malignancy should be made by other tests or tissue diagnosis. The major causes of false-positive results in lung patients are infectious, inflammatory and granulomatous disorders, and iatrogenic procedures, such as thoracocentesis, placement of a chest tube, percutaneous needle biopsy, mediastinoscopy, and talc pleurodesis.
Diagnosis of Pulmonary Nodules and Masses Peripheral solitary pulmonary nodules (SPNs) represent a diagnostic challenge, especially if they are noncalcified. With the increased interest in the use of low-dose spiral CT for early lung cancer detection, the number of coincidental SPNs will only increase.
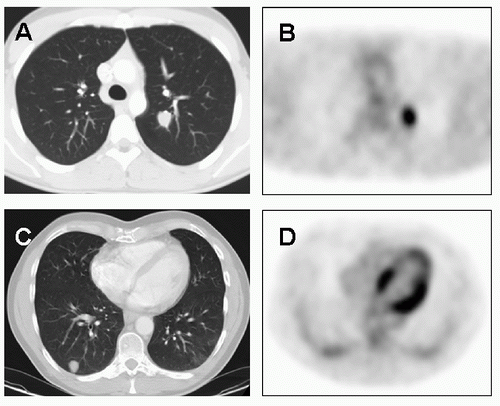
Multiple studies—often using a threshold maximum SUV (SUV max) of >2.5 for the diagnosis of malignancy—have proven the accuracy of PET in the differentiation of malignant from benign lesions (Fig. 27.2). In a metaanalysis, based on series with nearly all nodules larger than 1 cm, an overall sensitivity, specificity, positive and negative predictive value of 96%, 78%, 91%, and 92% was reported. 9
FIGURE 27.2 Solitary pulmonary nodule in the left upper lobe (A), with clear FDG uptake on PET (B). Surgery revealed pT1N0 adenocarcinoma. Solitary nodule in the right upper lobe (C), no uptake higher than lung background on PET (D). No change during follow-up, probably hamartoma.
False-negative findings may occur if a critical mass of metabolic active cells for detection on PET is not in place; therefore, exclusion of malignancy is more hazardous in small lesions.10 In that respect, the use of the SUVmax threshold of >2.5 should better be abandoned, because quite some lesions with SUVmax ≤2.5 are malignant. 11 A large prospective series (n = 585) looked at the accuracy of integrated PET/CT scan in SPNs ≤2.5 cm.12 If the SUV max was between 0 and 2.5, there was a 24% chance of malignancy; if between 2.6 and 4.0, it was 80%; and if >4, it was 96%. Likewise, the accuracy of PET is also challenged in small nodules detected in lung cancer screening studies. 13 Nonetheless, selective use of PET was reported to be useful in some series, 14,15,16 but with more limitations than in the daily practice population presenting with SPNs.
False-negative images are also common in tumors with low metabolic activity, bronchioloalveolar cell carcinomas in particular, 17,18 because they have significantly lower expression of the glucose transporter Glut-1 compared with other non-small cell lung cancer (NSCLC) subtypes. 19 Carcinoid tumors also have a low FDG uptake, 20,21 but the presence of somatostatin receptors in these neuroendocrine tumors allows PET imaging with radiolabeled somatostatine analogues, such as Ga-68-DOTATOC 22 (Fig. 27.1).
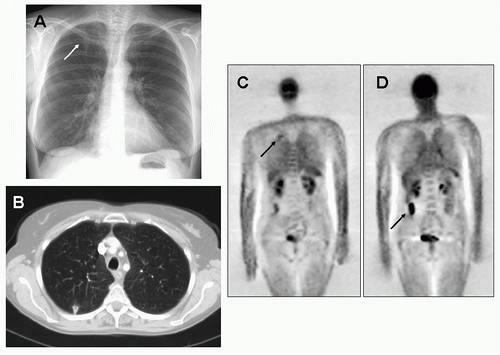
FIGURE 27.3 A 54-year-old woman in follow-up after radical radiotherapy for right vocal cord squamous cell carcinoma. Detection of a nodule in the right upper lobe on chest radiograph (A), confirmed at CT scan (B). PET showed some FDG avidity in the lesion (C), and in addition, a prominent FDG-positive lesion in the right hemicolon (D). Further studies pointed at postradiotherapy inflammation in the right lung and adenocarcinoma of the ascending colon.
False positives occur because of trapping of FDG in activated granulocytes and/or macrophages in several inflammatory conditions 23,24,25 (Fig. 27.3), and this leads to a variable specificity (50% to 100%) in different series, according to the prevalence of certain inflammatory or infectious diseases, such as tuberculosis or histoplasmosis. A nice pictorial overview of false-positive findings is given in Shim et al. 26 In special situations, specificity can be improved by looking at the FDG uptake kinetics using dual-time-point imaging at 1 and 2 hours (FDG continued uptake in malignant versus rapid uptake followed by washout in benign lesions). 27
Lung Cancer Staging CT, with its excellent anatomic detail, remains the method of choice to assess the T-factor, that is, the extent of the primary tumor in relation to lung fissures, mediastinal structures, pleura, or chest wall. PET on its own has little to add to the accuracy of CT because of its lower spatial resolution. 28 For the N-factor, one of the main limitations of CT—using only a size criterion—is its low accuracy in differentiating benign from malignant lymph nodes (LNs). 29,30 Since about a decade, PET i maging—with its metabolic information—was proven to be superior, 31,32 a finding confirmed in different metaanalyses based on a multitude of prospective studies. 33,34,35 PET on its own is more accurate, but is still not perfect in defining the N-status. Lack of anatomical detail is one important reason, for example, PET images often do not allow to distinguish hilar from mediastinal LNs (Fig. 27.4), or to exclude LNs in patients with a large centrally located tumor. Many well-designed prospective studies also demonstrated a gain in accuracy in the M-factor, mainly because PET is able to detect additional metastatic lesions in 5% to 25% of the patients. 36,37,38,39,40,41,42,43,44,45 There is a substantial variation in the proportion of patients with additional lesions, because authors differ in the definitions of “unexpected” lesions; in most series, an equivocal lesion on conventional imaging, found to be metastatic on PET, was not regarded as unexpected, although this was the case in some series. 37,40 If PET helps to characterize equivocal lesions, this is usually for adrenal lesions, contralateral lung nodules, or bone scintigraphy abnormalities. 36,37,38,40
Nowadays, the best combination of morphologic and metabolic information is obtained by integrated PET/CT scanners. Comparative results for the T-factor are listed in Table 27.3. Comparisons are often made with PET alone or with PET images in visual correlation with CT images. Although the first comparison may be of scientific interest, it is of little clinical relevance. Papers in the late 1990s already pointed out that interpretation of PET images in visual correlation with CT images was the minimum standard.31,46 Three studies reported better results with PET/CT in comparison with PET alone. 47,48,49 This superiority can be assigned to the CT component of this examination because of poor performance of PET alone in measuring tumor size or assessing potential infiltration of adjacent structures. The integrated images allow more precise evaluation of chest wall and mediastinal infiltration in some patients, and better differentiation between tumor and accompanying inflammation or atelectasis in others. In the Zurich group report, there was a benefit in comparison with side-by-side reading of PET and CT images as well, which was not in the place in the Leuven experience. 50 Results for the N-factor display a similar picture (Table 27.4), with PET/CT superior to PET alone. Accurate anatomic correlation allows exact location of involved nodes, and thus better distinction between N1, N2, and N3. Furthermore, the role of PET/CT in identifying supraclavicular N3 nodes and in the distinction between FDG-avid brown fat and a metastatic LN is indisputable 47,48,49 (Fig. 27.5). Here again, in the study of the Zurich group, PET/CT was superior to visual comparison, but the accuracy of the latter in this study was unexpectedly low at 59%. 47 In the Leuven experience, there was little difference between integrated and visually compared imaging, 50 confirming a similar previous experience with software fusion. 51 Finally, for the M-factor, only a few results are available. In a large retrospective study, there was a significant superiority of PET/CT versus PET alone or CT alone, but not versus sideto-side correlation. 28
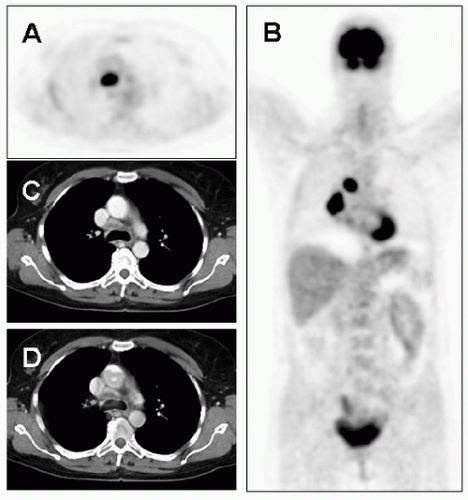
FIGURE 27.4 Transaxial (A) and coronal (B) PET images with a right lung tumor and accompanying adenopathy, either in the right hilar or mediastinal station. On CT, there is a suspect LN (C), on integrated PET/CT, right paratracheal adenopathy is confirmed (D). (See color plate.)
TABLE 27.3 Comparative Data on PET/CT regarding T-Stage