Population-Based Lung Cancer Prevention: An Overview
Population-Based Lung Cancer Prevention: An Overview
Anthony W. Kim
Mark A. Yoder
Michael J. Liptay
James L. Mulshine
Lung cancer remains the leading cause of cancer-related mortality in the United States, with 160,390 deaths projected for 2007.1 Lung cancer accounts for the largest number of cancer deaths worldwide as well, with an estimated 1.3 million deaths in 2005.2 These dismal numbers reflect persistent national and global challenges to lung cancer control.
Cancer control in general relies upon prevention, early detection, and treatment. Advances in the treatment of lung cancer, including minimally invasive surgery and targeted molecular therapies, have a limited impact on the burden of lung cancer because of the fact that most cancers continue to be diagnosed at an advanced stage. The presence of symptoms at the time of diagnosis is associated with a high probability of advanced disease. The failure of screening with chest radiography and sputum cytopathology to impact lung cancer mortality suggests that detection of asymptomatic disease is necessary but not sufficient to achieve this goal. A resurgence of interest in early detection has followed the widespread availability of chest computed tomography (CT). Although this technology has proven superior to chest radiography in detecting early stage lung cancers, a beneficial effect on lung cancer mortality remains to be proven.3 Smoking control programs continue to represent the most logical approach to curtailing lung cancer incidence, but economic and political forces oppose such efforts. 1 Reducing smoking prevalence decreases an individual smoker’s risk of lung cancer as well as that of others through a reduction in secondhand smoke exposure. Unfortunately, an elevated risk of lung cancer persists for many years after smoking cessation.4,5 This risk is highest among individuals who have undergone a curative resection for lung cancer, who have a 1% to 5% annual risk of developing a second primary lung cancer.6 Chemoprevention has been studied as a mechanism to decrease lung cancer risk in these high-risk groups as well as in the general population.
A population-based approach to lung cancer prevention will be required to achieve the greatest reduction in lung cancer mortality, as many individuals lack access to the healthcare system and may not otherwise be aware of their lung cancer risk. High-risk individuals must therefore be actively selected from the general population to ensure that the majority has the opportunity to receive appropriate preventive measures. Investigators have used such an approach to identify and recruit subjects into an ongoing chest CT screening trial,7 and we have previously reviewed the criteria for a population-based approach to early lung cancer detection.8 In contrast to breast or colon cancer, where the major defining risk factor is age, the profound risk associated with tobacco use allows for a powerful and economical additional selection factor to enrich for lung cancer risk. Other risk factors of lung cancer exist, however, and these collectively account for about 10% of lung cancer diagnoses. Which preventive measures should be applied to which specific subgroups of the population are questions that ongoing studies will help to address, but the answers will likely be dynamic as novel approaches are developed. This chapter will review contemporary lung cancer prevention strategies with a focus on their potential for implementation at a population level.
PREVENTION OF PRIMARY DISEASE
Smoking Cessation Lung cancer initially had a humble beginning, with early case reports remarking on the rarity of the disease. Only after the tremendous increase in smoking worldwide following World War I did lung cancer begin to achieve its current level of notoriety.9 Since the initial linkage between tobacco smoke and lung cancer in 1950,10,11 this risk factor has been extensively investigated. Smoking currently accounts for 87% of lung cancer deaths,12 and thus smoking cessation represents the most broadly applicable approach to primary prevention. Initiatives in the United States have only recently begun to result in a reduction in lung cancer mortality.3 One reason for this sluggish response is that a former smoker’s risk of lung cancer never returns to that of a nonsmoker.4,5 In fact, at present, about 50% of cancer diagnoses are made among former smokers.5,9 New medications may improve the success of individual smoking cessation attempts, but this rate remains below 10% over the long term with heavy smokers. Despite these limitations, tobacco control and smoking cessation remain key components of the primary prevention of lung cancer, with the long-term potential to banish this lethal disease back into obscurity. Lung cancer risk increases with duration of smoking. However, the increasing risk of lung cancer stops rising with smoking cessation.
Obstacles to Population-Level Smoking Cessation Initiatives Several obstacles stand in the way of smoking cessation initiatives. Smoking prevalence remains high. Worldwide smoking prevalence is 47% among men and 12% among women.9 An estimated 45 million Americans are current smokers, with a like number of former smokers.13 Adolescent smoking is also a persistent and serious problem. Tobacco addiction is not typically considered a pediatric disease, but data suggest that most adult smokers become addicted between age 13 and 17.9 With this background, the fact that about 30% of high school students report the use of some form of tobacco product within the previous month14 takes on greater significance. Secondhand smoke expands the reach of lung cancer to nonsmokers. About 126 million nonsmoking Americans are exposed to secondhand smoke in the workplace, home, vehicles, or public places,15 and about 3000 nonsmokers die of lung cancer as a result each year.16 Despite legally imposed limitations, the tobacco industry continues to advance its interests, with promotional expenditures exceeding tobacco control spending by a ratio of 23 to 1 in 2003. Declines in smoking cessation rates among adults and high school students appear to have stalled,17 likely as a consequence of increased industry marketing expenditures, decreased funding for comprehensive tobacco control programs, and lack of a significant increase in tobacco prices.18 While rates of smoking prevalence in other developed countries have largely mirrored the decline observed in the United States, increased marketing in the face of limited financial resources has resulted in increased tobacco consumption in developing countries.19
TABLE 15.1 Recommendations for Tobacco Control Initiatives1,19,20,21
Intervention
Effect(s)
Monitor tobacco use and prevention policies
Assesses control program and industry compliance
Protect people from tobacco smoke
Decreases tobacco consumption and smoking prevalence
–Comprehensive smoke-free laws
Offer help to quit tobacco use
Increases long-term smoking cessation rate
–National tobacco quit line
Expands access by underserved individuals
–Comprehensive coverage of counseling and pharmacotherapy
Warn about the dangers of tobacco smoke
Decreases tobacco consumption and smoking prevalence
–Antismoking media campaign
Enforce bans on advertising, promotion, and sponsorship
Decreases tobacco consumption
Raise taxes on tobacco
Decreases tobacco consumption
Provides funding for control program
Smoking cessation research
Discovers better interventions
System-based improvements
–Training of clinicians
–Systematic implementation by health systems
–Add smoking cessation as health systems quality indicator
Recommendations for Smoking Cessation Initiatives The U.S. Surgeon General’s report specified the goals of preventing tobacco use initiation among the young, promoting quitting, and eliminating nonsmokers’ exposure to secondhand smoke.1 A subcommittee of the U.S. Interagency Committee on Smoking and Health (ICSH), with public input, developed a national action plan consisting of ten recommendations for smoking cessation.20 The Centers for Disease Control and Prevention provided recommendations for the essential components of comprehensive tobacco control programs.21 The World Health Organization recently published its recommendations to curb the global smoking epidemic.19 These recommendations are summarized in Table 15.1, most of which will be discussed in more detail.
Youth Access Laws Laws aimed at restricting children and adolescents from purchasing tobacco products have not been very successful. Some studies suggest that such laws have no impact on adolescent smoking,22,23 whereas others demonstrate a decrease in the number of adolescents who experiment with smoking.24 Regardless, most smokers become addicted before they can purchase cigarettes legally.25 Lack of enforcement may largely explain the lack of efficacy of this approach.
Smoke-Free Laws As of January 2008, 26 states, encompassing 53% of Americans, had enacted or implemented legislation that prohibits smoking in the workplace, restaurants, or bars.26 However, only 5% of the global population is protected by smoke-free laws.19 Comprehensive public smoking bans are the most effective, with exposure to secondhand smoke being reduced from 46% in countries without regulations to 12% in those with extensive restrictions, but only to 35% in countries with limited restrictions.27 Additional benefits of such programs are a reduction in smoking prevalence and tobacco consumption by smokers, as well as lower rates of youth smoking specifically.15 A metaanalysis reported a 3.8% reduction in smoking prevalence and decrease by 3.1 cigarettes per day per continuing smoker. These results equate to a 29% reduction in cigarette consumption per employee. Public smoking bans decrease youth smoking prevalence, and school bans decrease daily consumption.22
Greece has the highest proportion (45%) of adult smokers in Europe. Many European countries have now adopted public smoking bans. Ireland was the first European country to implement a comprehensive ban on smoking in public places in March 2004. Norway followed soon after, but allowed a smokers’ corner in workplaces. Italy banned workplace smoking in January 2005 and Naples and Verona have made smoking illegal in public parks. Belgium allows smoking in cafes and bars if they have ventilation installed and are at least 50 sq m (538 sq ft) in area. In France, a law forbidding smoking in public places was extended to bars, cafes, and hotels in January 2008, with fines up to 450 euros (£332; $662). Eight German states, including Berlin, have also ushered banned smoking in 2008 declaring their pubs and restaurants smoke free. Almost a third of Germans smoke and the authorities in Berlin decided not to enforce the restrictions actively for the first 6 months.
In summary, highly restrictive smoke free laws have a tremendous potential to reduce smoking prevalence and tobacco consumption at the population level, but are underutilized even in developed countries.
Methods to Improve Individual Smoking Cessation Rates The rate of smoking cessation without any intervention is about 1% per year. This value varies by population, however, with this low rate being typical of smokers seen in a general medicine clinic. Higher baseline rates can be expected of individuals presenting to a smoking cessation clinic or following hospitalization for a smoking-related illness, such as myocardial infarction. Despite this discouraging figure, many smokers are motivated to make cessation attempts, with about 42% reporting at least one attempt in the prior 1 year.14,28 A significant opportunity exists for healthcare providers to intervene, as 70% of smokers visit their physicians annually. Physician counseling for only 2 to 3 minutes increases the rate of smoking cessation to 3%, making this intervention more cost-effective than treatment of dyslipidemia or mild-to-moderate hypertension. Tobacco quit lines are another means of providing counseling. Smokers are four times more likely to utilize a quit line than to seek help in person, and success rates of up to 20% can be achieved.20 Quit lines are toll free and thus expand the access of underserved populations to smoking cessation resources. Telephone counseling in more effective than mailed self-help materials,29 and personalized correspondence is superior to standardized letters.22 Pharmacologic therapy, in the form of nicotine replacement, bupropion, or varenicline, also improves long-term smoking cessation rates.30 Although counseling and pharmacotherapy are cost-effective when compared to other covered services,20 insurance coverage of smoking cessation treatments varies. Only 20% of employer-sponsored plans provide at least some coverage,31,32,33,34 Medicaid provides no coverage in 14 states,31 and Medicare only covers treatment of individuals with smoking-related diseases.35 Clearly, support for at least some of these interventions is a realistic goal for any country in the world.
Antismoking Media Campaigns Many smokers are not aware of the negative health consequences of smoking. Media campaigns offer a mechanism of providing education and countering specific misconceptions about smoking. Most recently, these campaigns have successfully targeted child and adolescent smoking. A media campaign coupled with a school-based program resulted in a decrease in reported smoking and weekly smoking in children in grades 4 through 6. Twelve-to thirteen-year-old individuals who reported seeing antismoking advertisements (ads) had half the chance of becoming established smokers as those who did not see the ads.24 A nationwide antismoking media campaign was credited with 22% of the decline in youth smoking between 1990 and 2002.36 Additional factors in this decline were restrictions on public smoking and an increase in the price of cigarettes.37,38,39 Securing the financial resources necessary to conduct large-scale antismoking media campaigns is a challenge, made more serious by expanded tobacco industry marketing in developing countries, but it can be offset or overcome in the following way.
Excise Taxes Imposing a tax on tobacco products has the potential to accomplish several goals. Currently, taxes are levied by state and local governments in the United States, resulting in striking disparities in the price of tobacco products across the country. Not surprisingly, most smokers obtain cigarettes in geographic locations with the lowest cost or employ other high-price avoidance strategies.40 This practice is associated with a lower probability of making a cessation attempt and possibly a lower quit rate.41 A federal tax on tobacco products would have the effect of equalizing their price, thereby preventing this evasion tactic. Imposing such a tax would have at least two other potential benefits. A 10% increase in cigarette price reduces consumption by 3% to 5%.42 This effect is more pronounced among economically disadvantaged individuals, including children and adolescents.20 Although smoking cessation is the preferred outcome, a reduction in consumption may decrease the risk of lung cancer. A 50% reduction in consumption among those smoking 15 or more cigarettes per day is associated with a 27% reduction in lung cancer risk.43 The second direct benefit is the revenue that these taxes generate, which is generally sufficient to fund other components of a comprehensive tobacco control program. Tobacco companies spend about $11 billion per year to offset these taxes.44
Outcomes of Comprehensive Tobacco Control Programs The fundamental measures employed by comprehensive tobacco control programs are excise taxes, antismoking media campaigns, and smoke-free laws. Results from two programs, in Massachusetts and New York, have been published. The Massachusetts Tobacco Control Program (MTCP) reduced consumption from 547 million packs to 280 million from 1992 to 2004, a decline of 4% per year. Even after adjustment for unequal increases in excise taxes, this decrease exceeded that of states that did not have control programs in place over the study period. Smoking prevalence decreased from 23.5% to 19.4% over 1990 to 1999. High school smoking prevalence decreased from 30.2% to 20.9% from 1993 to 2003. Smoking bans decreased exposure to smoking in the workplace from 44% to 15% from 1993 to 2001, in the home from 28% to 16%, and in restaurants from 64% to 37% from 1993 to 2002. 24 New York City’s program incorporated a tax increase, workplace smoking ban, and free nicotine patch program. These efforts resulted in an 11% reduction, from 21.6% to 19.2%, in smoking prevalence over 1 year, equating to 140,000 individuals who quit smoking. Forty-five percent of smokers reported cutting down, thinking about quitting, trying to quit, or quitting as a result of these initiatives. Forty-six percent of individuals reported less exposure to secondhand smoke following introduction of the program. The proportion of nonsmokers reporting secondhand smoke exposure at home decreased 29%, from 8.5% to 6%, equating to 105,000 fewer nonsmokers exposed. The proportion reporting workplace exposure decreased 18%, from 8.9% to 7.3%, a reduction of 67,000 nonsmokers exposed. Not surprisingly in a program implemented within a relatively narrow geographic region, purchases through alternative channels increased 89%, but nevertheless yielded a net reduction in consumption of 15%.45 A statewide ban on public smoking decreased exposure to secondhand smoke from 19.8% to 3.1% in restaurants and from 52.4% to 13.4% in bars in New York. Salivary cotinine levels, a marker of smoke exposure, decreased from 0.078 ng/mL to 0.041 ng/mL among nonsmokers.46 Overall findings from comprehensive tobacco control programs suggest that warning labels and advertising restrictions are less effective than increased taxes, smoking bans, and counteradvertising.22 Concordant with the results observed in Massachusetts, per capita cigarette purchases declined 16% to 20% in states implementing tax-supported antismoking programs.22
Impact on Lung Cancer Mortality Smoking prevalence fell from 42.3% to 23.2% in the United States between 1965 and 1997, but lung cancer incidence increased 230% between 1965 and 1999.9 This highlights the fact that lung cancer risk reduction is both delayed and incomplete following smoking cessation. The cumulative incidence of lung cancer through age 75 is about 16% for lifelong smokers, compared to less than 1% for lifelong nonsmokers. Smoking cessation at age 30, 40, or 50 years results in cumulative incidence rates of about 2%, 3%, and 6%, respectively. 47 These data indicate that a significant burden of lung cancer risk, and thus lung cancer mortality, can be eliminated by early smoking cessation, but that the risk never decreases to the level of a lifelong nonsmoker. This reality suggests that smoking cessation remains a critical prevention strategy; however, in an evolving situation where the number of former smokers whose significant lung cancer risk never normalizes, additional public health measures are required.48
Population-Based Screening Published lung cancer screening trials have generally involved current and former smokers. Family history may be an additional factor to consider when selecting the population to screen. A family history of lung cancer is an independent risk factor for lung cancer. The diagnosis of squamous cell carcinoma in a first-degree relative appears to confer the greatest risk.49 The risk of lung cancer in secondhand smoke-exposed individuals is measurable but significantly lower than in smokers. This means the potential cost benefit ratio will not be as favorable as for the smoking cohort and no prospective information addresses this circumstance as yet. Two large ongoing trials are accruing to address this issue (Flight Attendants Medical Research Institute, [FAMRI] and the International Early Lung Cancer Action Project [I-ELCAP]). Other risk factors for lung cancer include radon, asbestosis, certain metals (chromium, cadmium, arsenic), some organic chemicals, radiation, air pollution, tuberculosis, and genetic factors.1 Other approaches to early lung cancer detection have been reported such as with techniques to evaluate tobacco-exposed bronchial epithelial cells recovered in the sputum of smokers. An antibody against heterogeneous nuclear ribonucleoprotein A2/B1 has demonstrated high sensitivity and specificity for the detection of lung cancer in high-risk individuals.50,51,52 However, scaling such a test to achieve the requisite accuracy at affordable cost is a profound challenge given the comparable cost and availability of spiral CT screening.53
CHEMOPREVENTION
Lung cancer, like many other cancers, appears to be the final consequence of dysregulation involving varied pathways. However, this results in a common “phenotypic” outcome. Population-based lung cancer screening has yet to evolve into an established format. Looking forward, population-based screening could evolve as a multifaceted public health strategy, including successful youth-directed tobacco control, more effective smoking cessation for existing smokers, and integrated early detection, management, and chemoprevention for current and former smoker.
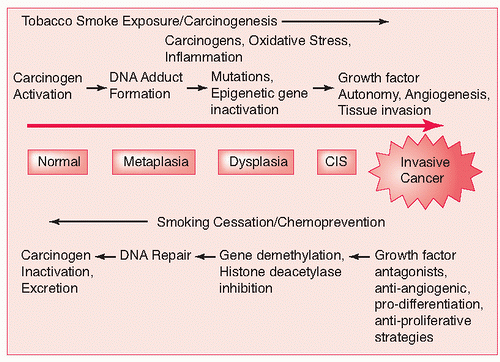
The conceptual basis for chemoprevention arises from the consideration of the long evolution of an epithelial cancer. This opportunity is best demonstrated by considering the colon cancer model. Multiple steps cumulatively define a continuum at the cellular level. These steps then served as watershed points at which more aggressive histopathologic progression could be identified and thereby mark the point at which cancer had evolved. In general, it is believed that lung cancer evolves by two potential pathways. The first involves the proliferation of aberrant cells that continue to devolve into carcinoma by sequential progression from hyperplasia through metaplasia and dysplasia. The second pathway involves “redifferentiation” or the dedifferentiation of bronchial epithelial cells that eventually redifferentiate into carcinoma.54 It is conceivable that combinations of both pathways at various points ultimately results in the phenotypic presentation of lung cancer.
FIGURE 15.1 Schematic representation of the e volution of normal bronchial epithelium to invasive lung cancer. (Reprinted with permission from Keith RL, Miller YE. Lung cancer: genetics of risk and advances in chemoprevention. Curr Opin Pulm Med 2005;11:265-271.)
The term chemoprevention was introduced by Sporn et al.55 in 1976 and was used to describe interventions used to slow or reverse progression of premalignant lesions to frank cancer. Targeting the “at-risk” population is crucial to the success of population-based chemoprevention. In lung cancer, chemoprevention strategies are targeted at the following three main groups:
Primary—chemoprevention among individuals at high risk who are otherwise healthy
Secondary—chemoprevention among individuals at high risk with premalignant conditions
Tertiary—chemoprevention among individuals with a known history of malignancy aimed at preventing second malignancies56
Chemoprevention agents encompass a tremendous number of potential natural and synthetic agents. These can be broadly subdivided into pharmaceutical, nutritional, and molecular targets. Each one of these broad categories can be f urther subdivided.
Chemoprevention Strategies Experimental work in rodents suggests that specific drugs can mitigate the progressive development of lung neoplasias after the exposure to specific tobacco-carcinogen exposures.57,58 Additional impetus arises from the clinical experience with antiestrogens in the chemoprevention of breast cancer. 59,60 However, the clinical development of these drugs is fraught with a number of challenges, including the protracted time and profound monetary resources required for such commercial development efforts. Defining objective surrogates of long-term outcomes has also been an unresolved challenge.61 As previously mentioned, it is largely held that a multistep carcinogenesis pathway exists from the normal bronchial epithelium to the frankly malignant tissue (Fig. 15.1). Along this pathway, changes from hyperplasia, atypia, metaplasia, and dysplasia are believed to occur and these changes are being utilized as surrogate end point biomarkers rather than frank carcinoma.62,63,64
Only gold members can continue reading. Log In or Register to continue